A client has been diagnosed with postpartum psychosis. Which of the following actions should the nurse take? Select one:
Maintain the client on strict bedrest.
Carefully monitor intake and output.
Restrict visitation of the client's partner.
Closely supervise all infant care and interaction.
The Correct Answer is D
Choice A Reason: Maintain the client on strict bedrest. This is an inappropriate action that may worsen the client's condition and increase her isolation and depression. Postpartum psychosis requires prompt psychiatric treatment with medication and psychotherapy, not bedrest.
Choice B Reason: Carefully monitor intake and output. This is an irrelevant action that has no direct relation to postpartum psychosis or its management. Monitoring intake and output may be indicated for other postpartum complications such as hemorrhage, infection, or preeclampsia.
Choice C Reason: Restrict visitation of the client's partner. This is an unnecessary action that may deprive the client of social support and emotional comfort. The partner may be an important source of help and information for the client and the health care team. The partner should be involved in the client's care and education, unless there are signs of abuse or violence.
Choice D Reason: Closely supervise all infant care and interaction. This is because postpartum psychosis is a severe mental disorder that occurs in some women after childbirth, which can cause delusions, hallucinations, paranoia, mood swings, confusion, and suicidal or homicidal thoughts. Postpartum psychosis can pose a danger to both the mother and the infant, as the mother may harm herself or the infant due to distorted perceptions or impulses. The nurse should closely supervise all infant care and interaction to ensure safety and prevent injury.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Rule out a suspected hydatidiform mole. This is an incorrect answer that describes an unlikely condition for this client. A hydatidiform mole is a type of gestational trophoblastic disease where abnormal placental tissue develops instead of a normal fetus. A hydatidiform mole can cause vaginal bleeding, hyperemesis gravidarum (severe nausea and vomiting), preeclampsia, and hyperthyroidism. A hydatidiform mole usually causes a fundal height measurement that is larger than expected for gestational age, not smaller.
Choice B Reason: Assess for congenital anomalies. This is an incorrect answer that implies that the client has not had a previous ultrasound to screen for fetal anomalies. Congenital anomalies are structural or functional defects that are present at birth, such as cleft lip, spina bifida, or Down syndrome. Ultrasound can detect some congenital anomalies by visualizing the fetal anatomy and morphology. However, ultrasound screening for fetal anomalies is usually done between 18 and 22 weeks of gestation, not at 32 weeks.
Choice C Reason: Determine fetal presentation. This is an incorrect answer that suggests that the client has an uncertain fetal presentation. Fetal presentation is the part of the fetus that is closest to the cervix, such as vertex (head), breech (butocks or feet), or transverse (shoulder). Fetal presentation can affect the mode and outcome of delivery. Ultrasound can determine fetal presentation by locating the fetal head and spine. However, fetal presentation can also be assessed by abdominal palpation or vaginal examination, which are simpler and less invasive methods.
Choice D Reason: Monitor fetal growth. This is because fundal height measurement is a method of estimating fetal size and gestational age by measuring the distance from the pubic symphysis to the top of the uterus (fundus) in centimeters. A fundal height measurement that is significantly smaller or larger than expected for gestational age may indicate intrauterine growth restriction (IUGR) or macrosomia, respectively. IUGR means that the fetal growth is slower than expected for gestational age, which can increase the risk of fetal distress, hypoxia, acidosis, and stillbirth. Macrosomia means that the fetal weight is higher than expected for gestational age, which can increase the risk of birth injuries, shoulder dystocia, cesarean delivery, and hypoglycemia. Ultrasound is a more accurate way of assessing fetal size and growth by measuring various parameters such as biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL). Ultrasound can also detect other factors that may affect fetal growth such as placental function, amniotic fluid volume, umbilical cord blood flow, and fetal anomalies.
Correct Answer is A
Explanation
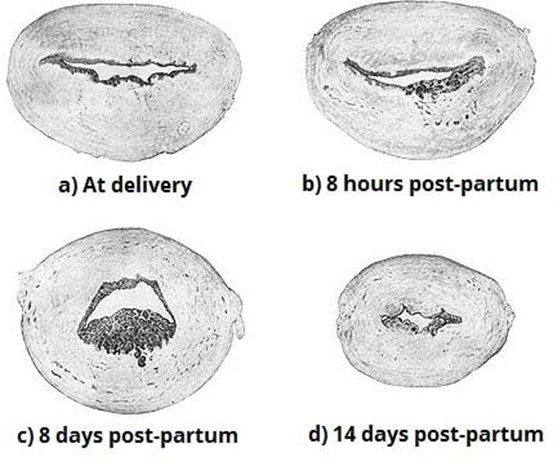
Choice A Reason: Inspecting the placenta after delivery for intactness. This is because inspecting the placenta after delivery for intactness is a nursing intervention that can prevent late postpartum hemorrhage, which is excessive bleeding from the uterus or genital tract that occurs more than 24 hours but less than 12 weeks after delivery. Late postpartum hemorrhage can be caused by retained placental fragments, subinvolution of the uterus, infection, or coagulation disorders. Inspecting the placenta after delivery for intactness can help identify and remove any retained placental fragments that may interfere with uterine contraction and involution, which are essential for hemostasis.
Choice B Reason: Manually removing the placenta at delivery. This is an incorrect answer that indicates an inappropriate and risky intervention that can cause late postpartum hemorrhage. Manually removing the placenta at delivery is a procedure that involves inserting a hand into the uterus and detaching the placenta from the uterine wall. Manually removing the placenta at delivery is indicated only for a retained or adherent placenta that does not separate spontaneously or with gentle traction within 30 minutes after delivery. Manually removing the placenta at delivery can cause trauma, infection, or incomplete removal of the placenta, which can increase the risk of late postpartum hemorrhage.
Choice C Reason: Administering broad-spectrum antibiotics prophylactically. This is an incorrect answer that suggests an unnecessary and ineffective intervention that can prevent late postpartum hemorrhage. Administering broad- spectrum antibiotics prophylactically is a pharmacological intervention that involves giving antibiotics to prevent or treat infection. Administering broad-spectrum antibiotics prophylactically is indicated for women with risk factors or signs of infection during or after delivery, such as prolonged rupture of membranes, chorioamnionitis, fever, or foul- smelling lochia. Administering broad-spectrum antibiotics prophylactically may reduce the risk of infection-related late postpartum hemorrhage, but it does not address other causes of late postpartum hemorrhage such as retained placental fragments or subinvolution of the uterus.
Choice D Reason: Applying traction on the umbilical cord to speed up separation of the placenta. This is an incorrect answer that refers to a different intervention that can prevent early postpartum hemorrhage, not late postpartum hemorrhage. Applying traction on the umbilical cord to speed up separation of the placenta is a technique that involves pulling on the umbilical cord while applying counter pressure on the uterus to facilitate placental expulsion. Applying traction on the umbilical cord to speed up separation of the placenta is indicated for active management of the third stage of labor, which can prevent early postpartum hemorrhage, which is excessive bleeding from the uterus or genital tract that occurs within 24 hours after delivery. Early postpartum hemorrhage can be caused by uterine atony, retained placenta, lacerations, or coagulation disorders.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today