A blind client reports that they are having difficulty with sleep that is affecting their daytime activities. Which of the following will the nurse include in her plan of care for the client?
Referral to a sleep study program
Assisting client to see if a night shift job is available
Institution of opioids and sedatives
Education about non-24 disorder
The Correct Answer is D
Choice A Reason: This is incorrect because a referral to a sleep study program is not the most appropriate plan of care for a blind client who has difficulty with sleep. A sleep study program is used to diagnose and treat sleep disorders such as sleep apnea, narcolepsy, or restless legs syndrome.
Choice B Reason: This is incorrect because assisting the client to see if a night shift job is available is not a helpful plan of care for a blind client who has difficulty with sleep. A night shift job can disrupt the circadian rhythm and worsen the sleep quality and quantity of the client.
Choice C Reason: This is incorrect because institution of opioids and sedatives is not a safe plan of care for a blind client who has difficulty with sleep. Opioids and sedatives can cause addiction, dependence, tolerance, and withdrawal symptoms. They can also impair the respiratory and cognitive functions of the client.
Choice D Reason: This is the correct choice because education about non-24 disorder is an essential plan of care for a blind client who has difficulty with sleep. Non-24 disorder is a condition where the internal clock of the body does not synchronize with the 24-hour day-night cycle. It can cause irregular sleep patterns, daytime fatigue, and mood disturbances. It is more common in blind people who lack light perception. The nurse should educate the client about the causes, symptoms, and treatments of non-24 disorder.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: This is correct because resuming a functional role in society is the ultimate goal for a client in the rehabilitative phase of a burn injury. The rehabilitative phase begins when wound healing is complete and lasts until physical and psychosocial recovery is achieved. The nurse should help the client regain independence, self-esteem, and quality of life by providing education, counseling, referrals, and resources.
Choice B reason: This is incorrect because pain management is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Pain management is important throughout all phases of burn care, but especially during wound healing and scar formation, which can cause itching, tightness, or hypersensitivity. The nurse should assess the client's pain level and administer analgesics, antipruritics, or moisturizers as ordered.
Choice C reason: This is incorrect because providing continued full support to the client is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Providing continued full support to the client can help them cope with physical and emotional challenges, such as scarring, disfigurement, disability, or depression. The nurse should provide emotional support, active listening, positive feedback, and encouragement to the client.
Choice D reason: This is incorrect because preventing infection is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Preventing infection is crucial during wound healing and grafting, which can be compromised by bacterial colonization or contamination. The nurse should monitor the client's vital signs, wound appearance, and laboratory results, and administer antibiotics or antiseptics as ordered.
Correct Answer is C
Explanation
Choice A reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
Choice B reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
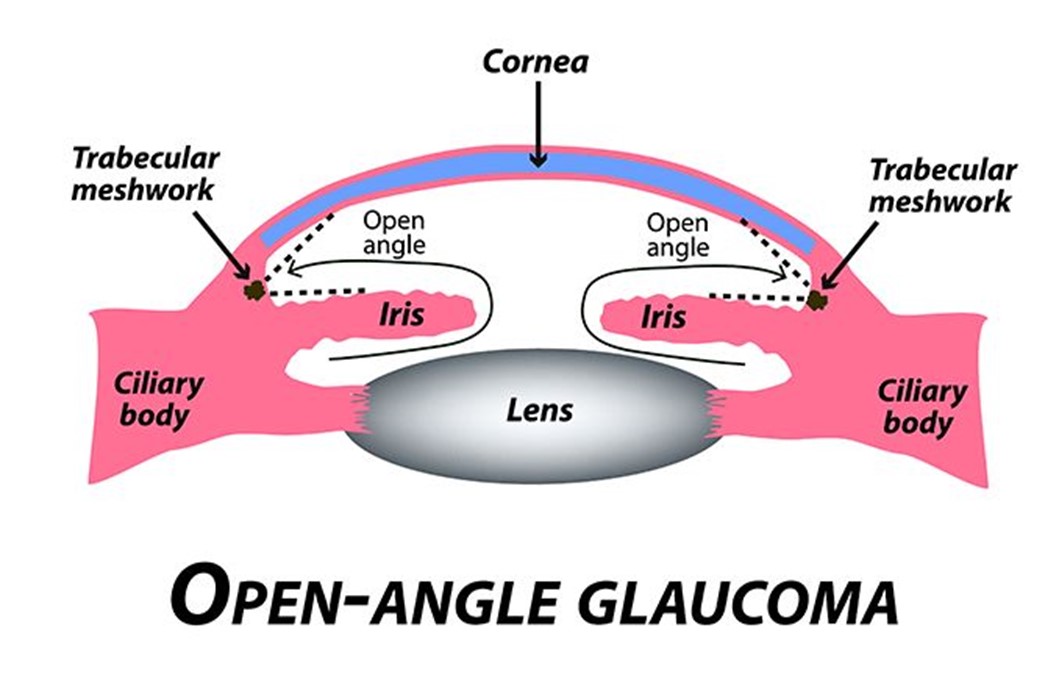
Choice C reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
Choice D reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today