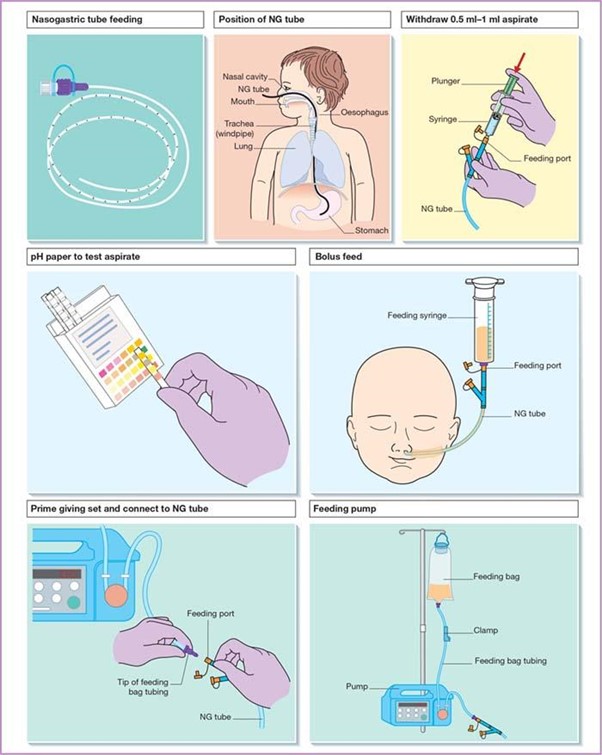
While assessing placement of a nasogastric tube (NGT), the nurse aspirates cloudy green fluid into a syringe. Which intervention should the nurse implement?
Send fluid specimen to the lab.
Withdraw the NGT and reinsert.
Connect the NGT to wall suction.
Determine pH value of specimen.
The Correct Answer is D
Choice A
This is unnecessary and not a standard clinical practice for confirming NGT placement.
Choice B
Withdrawing the NGT and reinsert should not be implemented. If the NGT is in the wrong place, reinserting it without further assessment could worsen the situation. The nurse should not reinsert the NGT until the correct placement is confirmed.
Choice C
Connecting the NGT to wall suction should not be implemented. Connecting the NGT to wall suction without verifying its placement could cause harm, especially if the tube is in the respiratory tract.
Choice D
This is the most evidence-based bedside method to confirm placement after the initial X-ray. Gastric aspirate typically has a pH of 5.0 or less. If the pH is higher (e.g., >6.0), it may indicate that the tube is in the lungs or the small intestine.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A
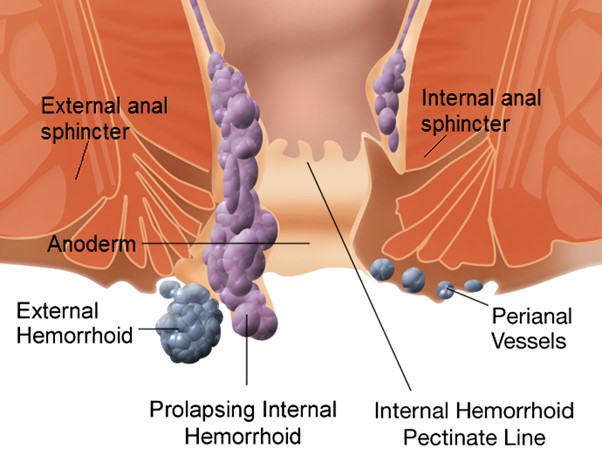
Explain the benefits of a high fibre diet is not correct response. While a high fibre diet can indeed be beneficial for individuals with haemorrhoids by promoting regular bowel movements and reducing strain during defecation, the immediate concern here is addressing the client's understanding about avoiding nuts and seeds. This information could be provided as a follow-up after confirming the client's understanding in response to option B.
Choice B
Confirm that these foods should be avoided is the correct response. In this situation, the nurse's first response should be to confirm the client's understanding and provide accurate information about the need to avoid certain foods. Nuts and seeds can be challenging to digest and may lead to irritation and inflammation in individuals with haemorrhoids. Confirming the client's understanding and providing guidance aligns with the nurse's role in patient education and care.
Choice C
Encourage soft foods such as yogurt is not the correct response. Encouraging soft foods like yogurt is a reasonable suggestion for someone with haemorrhoids, as soft foods are generally easier to digest and less likely to cause irritation. However, the client's statement was specifically about avoiding nuts and seeds. While this choice might be relevant, it doesn't directly address the client's statement.
Choice D
Suggest that the client also avoid fruit skins is not the correct response. This option is not directly related to the client's concern about nuts and seeds. Fruit skins generally contain dietary fibre, which can be beneficial for maintaining regular bowel movements. While some individuals might find that certain fruits with tough skins could exacerbate their haemorrhoid symptoms, this advice might be better suited for a separate discussion about dietary choices rather than as a direct response to the client's statement.
Correct Answer is B
Explanation
Choice A
Potatoes are incorrect. Potatoes are high in carbohydrates and can cause a rapid increase in blood sugar levels, so they are not the best choice for someone with diabetes trying to avoid refined sugars and carbs.
Choice B
Avocado is correct. Avocado is a good choice for someone with Type 2 diabetes who wants to avoid refined sugars and carbohydrates. Avocado is a healthy source of monounsaturated fats, fibre, and various vitamins and minerals. It has a low glycaemic index and doesn't significantly raise blood sugar levels, making it a suitable option for people with diabetes.
Choice C
Grapes is incorrect: Grapes are a fruit with natural sugars, and although they contain fibre, they can still cause spikes in blood sugar levels.
Choice D
Pretzels are incorrect. Pretzels are usually made from refined flour and are high in simple carbohydrates, causing rapid spikes in blood sugar levels. They are not a good choice for someone with diabetes aiming to avoid refined sugars and carbs.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today