Which sign or symptom would the nurse anticipate in a patient diagnosed with tuberculosis? Select all that apply. One, some, or all responses may be correct.
Weight gain
Low-grade fever
Dyspnea
Contusion
Lethargy
Night sweats
Correct Answer : B,C,E,F
Choice A Reason:
Weight gain is not typically associated with tuberculosis (TB). In fact, weight loss is a common symptom of TB due to the chronic nature of the infection and the body’s increased metabolic demands to fight the disease. Patients with TB often experience a loss of appetite and significant weight loss as the disease progresses.
Choice B Reason:
Low-grade fever is a common symptom of TB. The body’s immune response to the infection often results in a persistent low-grade fever, which can be one of the early signs of the disease. This fever is usually accompanied by other systemic symptoms such as night sweats and fatigue.
Choice C Reason:
Dyspnea, or difficulty breathing, can occur in patients with TB, especially if the infection has caused significant lung damage or if there is a large amount of fluid in the pleural space (pleural effusion). Dyspnea is a concerning symptom that indicates the need for further evaluation and treatment.
Choice D Reason:
Contusion, or bruising, is not a symptom associated with TB. TB primarily affects the lungs and can cause systemic symptoms, but it does not typically cause bruising. Contusions are more commonly associated with trauma or conditions that affect blood clotting.
Choice E Reason:
Lethargy, or a general sense of fatigue and weakness, is a common symptom of TB. The chronic nature of the infection and the body’s ongoing immune response can lead to significant fatigue. Patients with TB often feel tired and may have difficulty performing daily activities.
Choice F Reason:
Night sweats are a hallmark symptom of TB. Patients often experience drenching night sweats that can be quite severe. This symptom, along with fever and weight loss, is part of the classic triad of TB symptoms and is an important indicator for healthcare providers to consider TB in the differential diagnosis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason:
Constant bubbling in the water seal chamber of a chest drainage system typically indicates an air leak. This can occur if there is a break in the system, allowing air to enter. The air leak could be from the chest tube insertion site, the tubing, or the drainage system itself. Identifying and correcting the source of the air leak is crucial to ensure the system functions properly and the patient’s condition does not worsen.
Choice B Reason:
A tension pneumothorax is a life-threatening condition where air accumulates in the pleural space and cannot escape, leading to increased pressure on the lungs and other thoracic structures. While a tension pneumothorax can cause significant respiratory distress, it is not typically indicated by constant bubbling in the water seal chamber. Instead, signs of tension pneumothorax include tracheal deviation, hypotension, and severe respiratory distress.
Choice C Reason:
A kink in the tubing of a chest drainage system can obstruct the flow of air and fluid, but it does not cause constant bubbling in the water seal chamber. Instead, a kink would likely result in a lack of drainage or intermittent bubbling as the obstruction temporarily blocks and then allows passage of air or fluid.
Choice D Reason:
Increased drainage in a chest tube system indicates that more fluid or air is being removed from the pleural space, but it does not cause constant bubbling in the water seal chamber. Increased drainage might be seen in cases of hemothorax or pleural effusion, where large amounts of fluid are present.
Choice E Reason:
Tidaling refers to the normal rise and fall of water in the water seal chamber with the patient’s respiratory cycle. It indicates that the chest tube is patent and functioning correctly. Absence of tidaling could suggest that the lung has fully re-expanded or that there is an obstruction in the system. However, tidaling itself does not cause constant bubbling.
Correct Answer is A
Explanation
Choice A Reason:
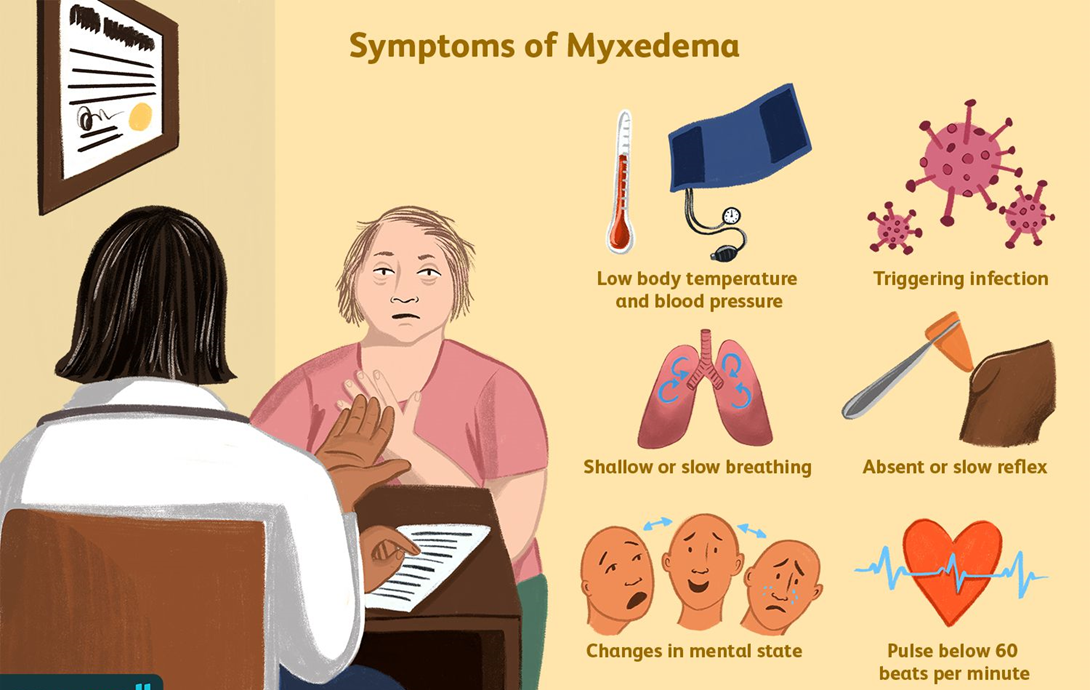
Place the client on aspiration precautions: Myxedema coma is a severe form of hypothyroidism that can lead to decreased mental function and a reduced level of consciousness. These conditions increase the risk of aspiration, which can lead to pneumonia and other complications. Therefore, placing the client on aspiration precautions is crucial to prevent these risks. Aspiration precautions may include elevating the head of the bed, monitoring swallowing ability, and providing thickened liquids if necessary.
Choice B Reason:
Turn the client every 4 hours: While turning the client regularly is important to prevent pressure ulcers, it is not the primary action needed for a client in a myxedema coma. The focus should be on stabilizing the client’s condition and preventing life-threatening complications such as aspiration, respiratory failure, and cardiovascular collapse.
Choice C Reason:
Check the client’s blood pressure every 2 hours: Monitoring vital signs, including blood pressure, is essential for clients in a myxedema coma. However, it is not the most critical action compared to preventing aspiration. Blood pressure should be monitored regularly, but the frequency can be adjusted based on the client’s condition and stability.
Choice D Reason:
Initiate measures to cool the client: Clients in a myxedema coma typically present with hypothermia (low body temperature), not hyperthermia (high body temperature). Therefore, initiating measures to cool the client would be inappropriate and could worsen their condition. Instead, measures to warm the client, such as using blankets and adjusting room temperature, are more appropriate.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today