Which actions should the practical nurse (PN) include when assessing a client for signs and symptoms of fluid volume excess? (Select all that apply.)
Palpate the rate and volume of the pulse.
Check fingernails for the presence of clubbing.
Measure body weight at the same time daily.
Observe the color and amount of urine.
Compare muscle strength of both arms.
Correct Answer : A,C,D
The PN should palpate the rate and volume of the pulse, measure body weight at the same time daily, and observe the color and amount of urine when assessing a client for signs and symptoms of fluid volume excess. These actions can help detect changes in the cardiovascular, renal, and fluid balance systems that may indicate fluid overloads, such as tachycardia, bounding pulse, weight gain, edema, oliguria, or dark urine.
The other options are not correct because:
B. Checking fingernails for the presence of clubbing is not relevant for assessing fluid volume excess, as clubbing is a sign of chronic hypoxia or lung disease that causes enlargement of the fingertips and nails.
E. Comparing muscle strength of both arms is not relevant for assessing fluid volume excess, as muscle weakness is not a specific sign of fluid overload, but may be caused by various factors such as electrolyte imbalance, nerve damage, or fatigue.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
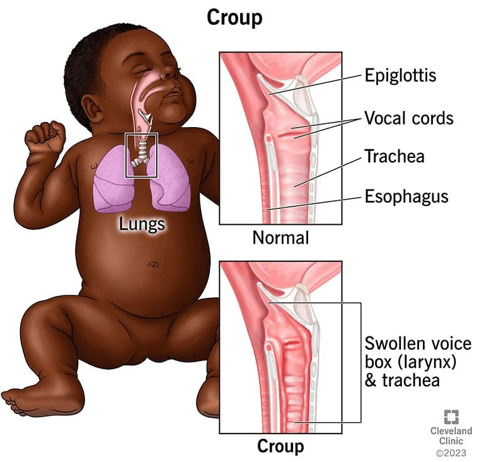
Croup is a respiratory infection that causes inflammation and narrowing of the airway, resulting in a barking cough, hoarseness, and stridor. The PN should monitor the child's oxygen saturation level via pulse oximetry, as it can indicate the severity of the airway obstruction and the need for supplemental oxygen or other interventions.
Correct Answer is ["A","B","D"]
Explanation
They are needed to remove the saline lock safely and prevent bleeding or infection. The PN should wear exam gloves to protect themselves and the client from contamination, apply a small gauze pad over the insertion site, and secure it with paper tape after removing the saline lock.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today