Upon entering the room of a client who has had a spontaneous abortion, the nurse observes the client crying. Which response by the nurse would be most appropriate?
I'm sorry you lost your baby.
Why are you crying?
Will a pill help your pain?
A baby still wasn't formed in your womb.
The Correct Answer is A
Choice A Reason: This is the correct answer because it is an empathetic and supportive response that acknowledges the client's loss and grief. This is an empathetic and supportive response that acknowledges the client's loss and grief. The other choices are inappropriate because they are insensitive, dismissive, or inaccurate.
Choice B Reason: This is an inappropriate answer because it implies that the nurse does not understand or care about the client's emotional state. It also suggests that the client has no Reason to cry, which is invalidating and hurtful.
Choice C Reason: This is an inappropriate answer because it focuses on the physical pain rather than the emotional pain of the client. It also implies that the nurse wants to avoid dealing with the client's feelings and just give them a medication to make them stop crying.
Choice D Reason: This is an inappropriate answer because it is inaccurate and misleading. A spontaneous abortion, also known as a miscarriage, occurs when a pregnancy ends before 20 weeks of gestation. At this stage, the baby is already formed and has a heartbeat, organs, and limbs. Saying that a baby still wasn't formed in the womb is false and insensitive to the client's loss.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
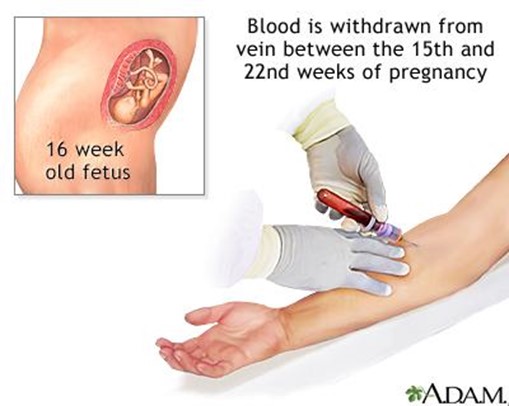
Choice A Reason: This is incorrect because sickle-cell anemia is a genetic disorder that affects the shape and function of red blood cells. It does not affect the AFP level, which is a protein produced by the fetus and placenta. Sickle-cell anemia can be detected by other prenatal tests, such as hemoglobin electrophoresis or DNA analysis.
Choice B Reason: This is incorrect because cardiac defects are structural abnormalities of the heart or blood vessels that affect the blood flow and oxygen delivery to the fetus. They may cause an increased AFP level, not a decreased one, as they can lead to fetal distress or edema. Cardiac defects can be detected by other prenatal tests, such as fetal echocardiography or ultrasound.
Choice C Reason: This is correct because Down syndrome is a chromosomal disorder that results from an extra copy of chromosome 21. It causes various physical and mental developmental delays and defects in the fetus. It is associated with a decreased AFP level, as well as decreased levels of human chorionic gonadotropin (hCG) and unconjugated estriol (uE3). Down syndrome can be confirmed by other prenatal tests, such as amniocentesis or chorionic villus sampling (CVS).
Choice D Reason: This is incorrect because respiratory disorders are problems that affect the breathing and gas exchange of the fetus. They may cause an increased AFP level, not a decreased one, as they can lead to fetal distress or edema. Respiratory disorders can be detected by other prenatal tests, such as fetal biophysical profile (BPP) or nonstress test (NST).
Correct Answer is B
Explanation
Choice A Reason: Linea nigra is a dark vertical line that appears on the abdomen of some pregnant women. It is caused by increased melanin production and usually fades after delivery.
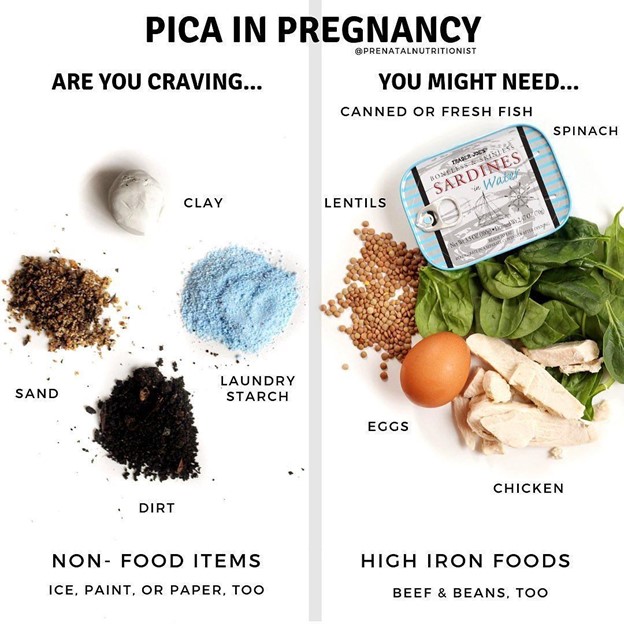
Choice B Reason: Pica is a condition in which a person has an abnormal desire to eat substances that are not food, such as ice, clay, dirt, or chalk. It is more common in pregnant women and may indicate a deficiency in iron or other nutrients.
Choice C Reason: Ballottement is a technique of palpating a floating structure by bouncing it gently and feeling it rebound. In obstetrics, it can be used to detect the presence of the fetus by feeling its head move when the cervix is tapped.
Choice D Reason: Quickening is the first perception of fetal movements by the pregnant woman. It usually occurs between 16 and 20 weeks of gestation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today