This is the edited text:
An nurse is caring for a client who is postoperative following an open reduction internal fixation (ORIF) of a femur fracture. What is included in the evaluation of the neurovascular status of the client's affected extremity? (Select all that apply.)
Color
Temperature
Ecchymosis
Skin integrity
Sensation
Correct Answer : A,B,E
Choice A reason: Color is an important indicator of the blood flow and oxygenation to the affected extremity. The nurse should compare the color of the skin, nails, and mucous membranes of the affected and unaffected extremities and look for any signs of pallor, cyanosis, or mottling. These signs can indicate ischemia, hypoxia, or impaired circulation, which can lead to tissue damage or necrosis.
Choice B reason: Temperature is another important indicator of the blood flow and oxygenation to the affected extremity. The nurse should compare the temperature of the skin of the affected and unaffected extremities by palpating with the back of the hand and look for any signs of warmth or coolness. These signs can indicate inflammation, infection, or reduced perfusion, which can affect the healing process or cause complications.
Choice C reason: Ecchymosis is not an indicator of the neurovascular status of the affected extremity. Ecchymosis is the discoloration of the skin caused by bleeding under the skin, which can result from trauma, surgery, or anticoagulant therapy. Ecchymosis is expected after an ORIF of a femur fracture and does not necessarily indicate a problem with the blood flow or oxygenation to the extremity.
Choice D reason: Skin integrity is not an indicator of the neurovascular status of the affected extremity. Skin integrity is the condition of the skin and its ability to resist damage, infection, or breakdown. Skin integrity can be affected by factors such as pressure, friction, moisture, or foreign bodies. The nurse should assess the skin integrity of the affected extremity and look for any signs of wounds, ulcers, or infections, but these signs do not reflect the neurovascular status of the extremity.
Choice E reason: Sensation is an important indicator of the nerve function and innervation of the affected extremity. The nurse should assess the sensation of the affected extremity by asking the client to report any numbness, tingling, or pain, or by testing the client's response to light touch, pressure, or temperature. These signs can indicate nerve damage, compression, or irritation, which can affect the mobility and function of the extremity.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
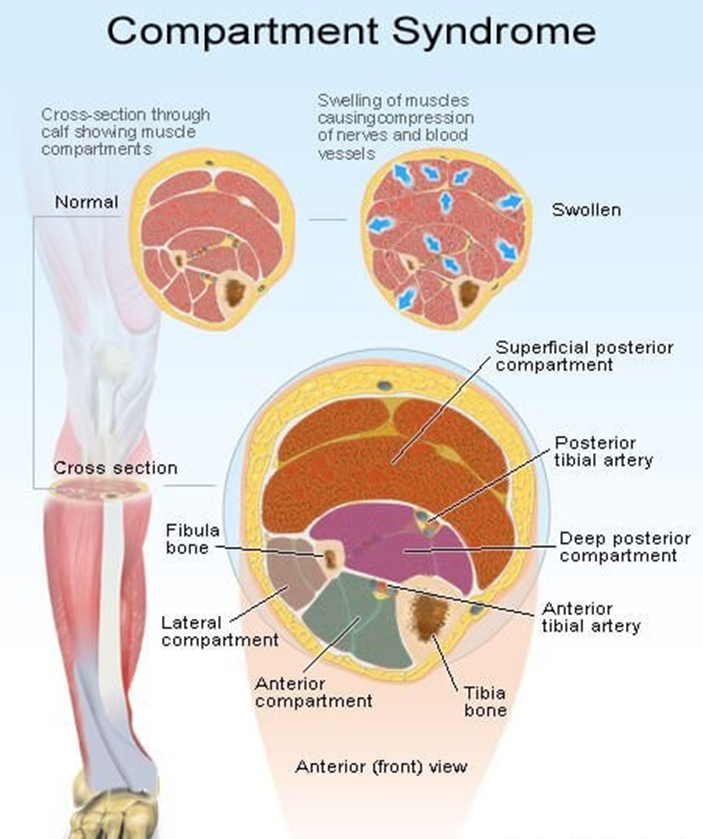
Choice A reason: A bone fragment has injured the nerve supply in the area is not the best response by the nurse. This may be a possible complication of a fracture, but it does not explain the mechanism of compartment syndrome. Compartment syndrome is a condition where the pressure within a closed space (such as a muscle compartment) exceeds the perfusion pressure and causes ischemia and necrosis of the tissues. A bone fragment may damage the nerve, but it does not cause increased pressure in the compartment.
Choice B reason: An injured artery causes impaired arterial perfusion through the compartment is not the best response by the nurse. This may be a possible cause of compartment syndrome, but it is not the most common one. Compartment syndrome is more often caused by venous obstruction than arterial obstruction. An injured artery may reduce the blood flow to the compartment, but it does not cause increased pressure in the compartment.
Choice C reason: Bleeding and swelling cause increased pressure in an area that cannot expand is the best response by the nurse. This is the most common cause of compartment syndrome and explains the pathophysiology of the condition. Bleeding and swelling are the result of inflammation and tissue injury that occur after a fracture. They increase the volume of fluid in the compartment, which cannot expand due to the rigid fascia that surrounds it. This leads to increased pressure in the compartment, which compresses the blood vessels, nerves, and muscles and causes ischemia and necrosis of the tissues.
Choice D reason: The fascia expands with injury, causing pressure on underlying nerves and muscles is not the best response by the nurse. This is not a correct statement, as the fascia does not expand with injury. The fascia is a tough connective tissue that encloses the muscle compartments and limits their expansion. The fascia is part of the problem, not the cause, of compartment syndrome. The fascia prevents the compartment from accommodating the increased volume of fluid and causes increased pressure in the compartment.
Correct Answer is B
Explanation
Choice A reason: Creating a susceptible host is not a way to break the chain of infection, but rather a way to facilitate it. A susceptible host is someone who is vulnerable to infection due to factors such as age, immunocompromised status, or chronic diseases.
Choice B reason: Maintaining the integrity of a portal of entry is a way to break the chain of infection, because it prevents the entry of microorganisms into the body. A portal of entry is any place where microorganisms can enter the body, such as the skin, mucous membranes, or respiratory tract. By reducing skin breakdown, the nurse is protecting the skin from becoming a portal of entry for infection.
Choice C reason: Creating a reservoir to decrease the risk of infection is a contradiction, because a reservoir is a place where microorganisms can multiply and survive, such as a human, animal, or environment. A reservoir increases the risk of infection, not decreases it.
Choice D reason: Sterilizing the area to reduce the reservoir risk is a way to break the chain of infection, but it is not related to reducing skin breakdown. Sterilizing the area means killing or removing all microorganisms from a surface or object, such as a surgical instrument or a wound dressing. This can reduce the reservoir risk, but it does not affect the integrity of the skin as a portal of entry.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today