The nurse is providing discharge teaching to a client after a total hip replacement. The teaching should include instructions to:
Avoid crossing the legs while sitting.
Eliminate Vitamin K from the diet.
Follow a home exercise program.
Use a raised toilet seat.
Increase high-impact activities.
Correct Answer : A,C,D
Choice a reason:
Avoiding crossing the legs while sitting is crucial after a total hip replacement to prevent dislocation of the new joint. Crossing the legs can put undue pressure on the hip joint and may lead to misalignment or increased strain during the healing process.
Choice b reason:
Eliminating Vitamin K from the diet is not typically recommended after a total hip replacement. Vitamin K is essential for blood clotting, and maintaining a consistent intake is important, especially if the client is on anticoagulant therapy to prevent deep vein thrombosis. Sudden changes in Vitamin K intake can affect the efficacy of anticoagulants like warfarin.
Choice c reason:
Following a home exercise program is an essential part of recovery after a total hip replacement. Exercises help strengthen the muscles around the new joint, improve flexibility, and increase range of motion. It's important that these exercises are done regularly and as instructed by a physical therapist.
Choice d reason:
Using a raised toilet seat after hip replacement surgery helps to prevent excessive flexion at the hip, which can risk dislocating the new joint. It also makes it easier for the client to sit down and stand up with less strain on the hip.
Choice e reason:
Increasing high-impact activities is not recommended after a total hip replacement, especially in the early stages of recovery. High-impact activities can put excessive stress on the new joint and may lead to complications. Low-impact activities such as walking, swimming, or cycling are generally more appropriate.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason:
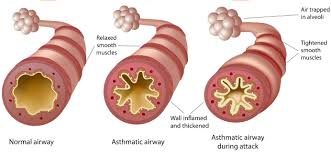
Using accessory muscles while breathing is a sign of respiratory distress and indicates that the client is working harder to breathe. This is not a desired outcome of treatment and suggests that the asthma exacerbation is not under control.
Choice B Reason:
The ability to answer questions in full sentences suggests that the client's airway is not severely obstructed, which is a positive sign of effective asthma treatment. When asthma is well-controlled, individuals should not experience significant shortness of breath that limits their ability to speak.
Choice C Reason:
Diminished breath sounds can be a sign of severe airway obstruction and are not indicative of effective asthma treatment. Ideally, lung auscultation should reveal clear breath sounds without wheezing, indicating good air movement throughout the lungs.
Choice D Reason:
Restlessness and anxiety can be symptoms of hypoxia, a condition where the body or a region of the body is deprived of adequate oxygen supply. This is not a sign of effective asthma treatment and may indicate that the client's asthma is not well-managed.
Correct Answer is A
Explanation
Choice A Reason
Acute compartment syndrome occurs when bleeding or swelling within an enclosed bundle of muscles – known as a muscle compartment – leads to increased pressure. This pressure can impede blood flow to the body tissue and destroy function. The fascia, which is a tough layer of fibrous tissue, does not stretch easily, so any swelling or bleeding can quickly lead to increased pressure.
Choice B Reason
While displaced bones can compress nerves and vessels, this is not the primary mechanism of acute compartment syndrome. Displaced bones are more likely to cause direct injury or impingement, but compartment syndrome specifically refers to the pressure build-up within a muscle compartment that affects circulation and tissue viability.
Choice C Reason
Interruption of blood supply to the bone is a serious concern and can lead to conditions such as avascular necrosis. However, in the context of acute compartment syndrome, the primary issue is the pressure within the muscle compartment rather than direct disruption of blood supply to the bone.
Choice D Reason
Compression of muscle tissue can restrict blood flow to the area, which is a part of the pathophysiology of compartment syndrome. However, the compression is a result of increased pressure within the compartment, not the primary cause. The increased pressure is due to bleeding and swelling, which is why choice A is the most accurate description.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today