The nurse is caring for a client who reports a sudden, severe headache, and facial numbness.The nurse asks the client to smile and observes an uneven smile with a facial droop to the right side and a hand grasp strength that is weaker on the right than the left. The client denies a recent history of headaches or trauma. After obtaining vital signs, the nurse should implement which intervention?
Place an indwelling urinary catheter and measure strict intake and output.
Maintain elevated positioning of the dependent joints on affected side.
Raise the head of the bed to 30 degrees keep head and neck in neutral alignment.
Determine when symptoms began and if improved or worsened since onset.
The Correct Answer is D
A) Incorrect- While monitoring urinary output is important for overall assessment, it is not the most critical intervention in this situation of suspected stroke. The client's neurological symptoms take precedence.
B) Incorrect- Positioning might be relevant to preventing complications, but it is not the highest priority intervention in this situation. The focus should be on assessing the client's neurological status and determining appropriate intervention.
C) Incorrect- Although head positioning is relevant for intracranial pressure management, it is not the immediate priority. The nurse should first assess the time of symptom onset and determine if the client is experiencing an acute stroke.
D) Correct- The client's symptoms, including sudden severe headache, facial numbness, facial droop, and weakness on one side, are suggestive of a stroke. The nurse should prioritize assessing the time of symptom onset, as time is a crucial factor in determining the appropriate intervention. Rapid intervention can improve outcomes in stroke cases, especially when considering interventions like thrombolytic therapy. The other options are not as directly relevant to the immediate management of a suspected stroke.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
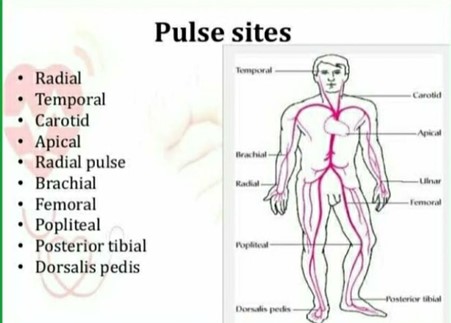
- A radial pulse is the pulse felt at the wrist, where the radial artery runs along the thumb side of the forearm. It is one of the most common sites for measuring a person's heart rate.
- To measure a radial pulse, the examiner should place two or three fingers over the radial artery, just below the wrist crease, and apply gentle pressure until a pulsation is felt. The examiner should not use the thumb, as it has its own pulse and may interfere with the accuracy of the measurement. The examiner should count the number of beats for 15, 30, or 60 seconds, depending on the regularity and rate of the pulse.
- In the picture, the unlicensed assistive personnel (UAP) is using the thumb to measure the radial pulse, which is incorrect. The practical nurse (PN) should demonstrate the correct pulse site to the UAP and explain why using the thumb is not appropriate. This will help to ensure that the UAP obtains an accurate and reliable pulse rate for the client.
Therefore, option C is the correct answer, while options A, B, and D are incorrect.
Option A is incorrect because instructing the UAP to report any abnormal findings does not address the error in technique.
Option B is incorrect because reminding the UAP to check the pulse volume does not address the error in technique.
Option D is incorrect because confirming the accuracy of the pulse rate obtained by the UAP does not address the error in the technique.
Correct Answer is B
Explanation
A) Incorrect- While a second IV site might be considered if the first one is causing significant discomfort, it's not the initial intervention. The nurse should first address the immediate concern of pain.
B) Correct- Pain at the IV site during infusion might indicate infiltration or irritation. Stopping the infusion is the most immediate intervention to prevent further discomfort and potential complications like tissue damage.
C) Incorrect- While assessing for blood return is important to ensure proper IV placement, it's not the initial intervention for managing pain caused by the infusion.
D) Incorrect- Discontinuing the IV might be considered if the pain is severe and unmanageable, but the nurse should initially try to address the discomfort without removing the IV.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today