The nurse identifies several nursing problems for a client with paraplegia who has been having fecal incontinence and diarrhea. The client's parent is the primary caregiver. In planning care, the nurse should determine which problem is the highest priority?
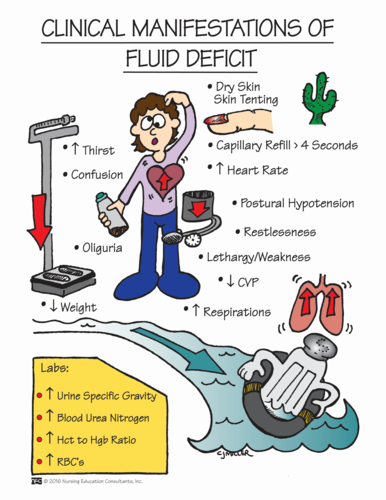
Fluid volume deficit.
Bowel incontinence.
Caregiver role strain.
Impaired bed mobility.
The Correct Answer is A
Choice A Reason: This is correct because fluid volume deficit is a life-threatening condition that can result from diarrhea and fecal incontinence. The nurse should monitor the client's fluid intake and output, electrolytes, weight, urine specific gravity, and skin turgor.
Choice B Reason: This is incorrect because bowel incontinence is a significant problem that can affect the client's dignity, comfort, and skin integrity, but it is not as urgent as fluid volume deficit. The nurse should implement a bowel management program and provide appropriate hygiene and skin care.
Choice C Reason: This is incorrect because caregiver role strain is a potential problem that can affect the parent's well-being and ability to provide care, but it is not as critical as fluid volume deficit. The nurse should assess the parent's coping skills, support system, and respite needs.
Choice D Reason: This is incorrect because impaired bed mobility is a chronic problem that can affect the client's functional status and quality of life, but it is not as serious as fluid volume deficit. The nurse should assist the client with positioning, turning, transferring, and exercising.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: This is correct because fluid volume deficit is a life-threatening condition that can result from diarrhea and fecal incontinence. The nurse should monitor the client's fluid intake and output, electrolytes, weight, urine specific gravity, and skin turgor.
Choice B Reason: This is incorrect because bowel incontinence is a significant problem that can affect the client's dignity, comfort, and skin integrity, but it is not as urgent as fluid volume deficit. The nurse should implement a bowel management program and provide appropriate hygiene and skin care.
Choice C Reason: This is incorrect because caregiver role strain is a potential problem that can affect the parent's well-being and ability to provide care, but it is not as critical as fluid volume deficit. The nurse should assess the parent's coping skills, support system, and respite needs.
Choice D Reason: This is incorrect because impaired bed mobility is a chronic problem that can affect the client's functional status and quality of life, but it is not as serious as fluid volume deficit. The nurse should assist the client with positioning, turning, transferring, and exercising.
Correct Answer is D
Explanation
Choice A: Have the client hold a pillow over the abdomen to cough and deep breathe is not the most important instruction because it is not related to repositioning. This is a good practice to prevent respiratory complications after surgery, but it can be done at any time.
Choice B: Encourage the client to eat all of the meals that are sent is not the most important instruction because it is not related to repositioning. This is a good practice to promote nutrition and healing after surgery, but it can be done at any time.
Choice C: Offer fruit juice at least twice during both the day and evening shifts is not the most important instruction because it is not related to repositioning. This is a good practice to prevent dehydration and constipation after surgery, but it can be done at any time.
Choice D: Lower the bed prior to helping the client to move up in bed is the most important instruction because it reduces the risk of injury and falls for both the client and the UAP. This is a safety measure that should be done before any repositioning.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today