The nurse begins collecting the medical history of a child when the child screams and tries to hide behind the parent, dropping a stuffed toy. Which intervention should the nurse implement?
Obtain the essential information as quickly as possible.
Document interactions between the parent and the child.
Ignore the child's behavior, directing questions to a parent.
Include the child's toy in the collection of information.
The Correct Answer is D
The nurse should implement the intervention of including the child's toy in the collection of information when the child screams and tries to hide behind the parent, dropping a stuffed toy. This can help engage the child and make them feel more comfortable during the medical history collection process. The other options (A, B, and C) are not appropriate interventions in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
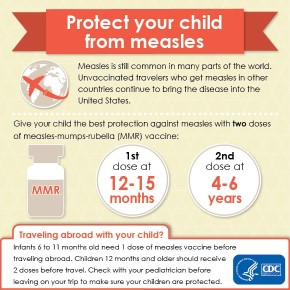
The American Academy of Pediatrics (AAP) and the Centers for Disease Control and Prevention (CDC) recommend that the first dose of MMR vaccine be given at 12-15 months of age.
A. 6 months is too early for the MMR vaccine.
D. 2 months is also too early for the MMR vaccine.
C. 24 months is slightly beyond the recommended range for the first dose of MMR vaccine, which is given between 12-15 months of age.
Correct Answer is C
Explanation
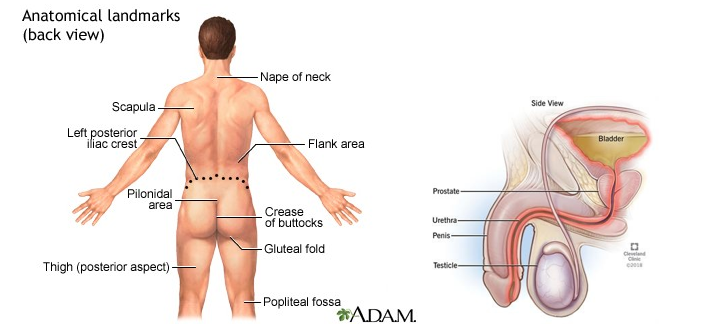
To determine a possible urinary tract infection in a preschool-aged child who presents with flank pain, dysuria, and low-grade fever, the nurse should gather additional information from the parent about new onset bedwetting. New onset bedwetting can be a sign of a urinary tract infection in children. The other options (A, B, and D) are not directly related to determining a possible urinary tract infection in this situation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today