A nurse in a provider's office is assessing a client who reports shoulder pain. Which of the following findings by the nurse indicates a rotator cuff injury?
Inability to abduct the arm at the shoulder.
Negative drop arm test.
Alteration in the contour of the joint.
A positive Tinel's sign.
The Correct Answer is A
Choice A reason:
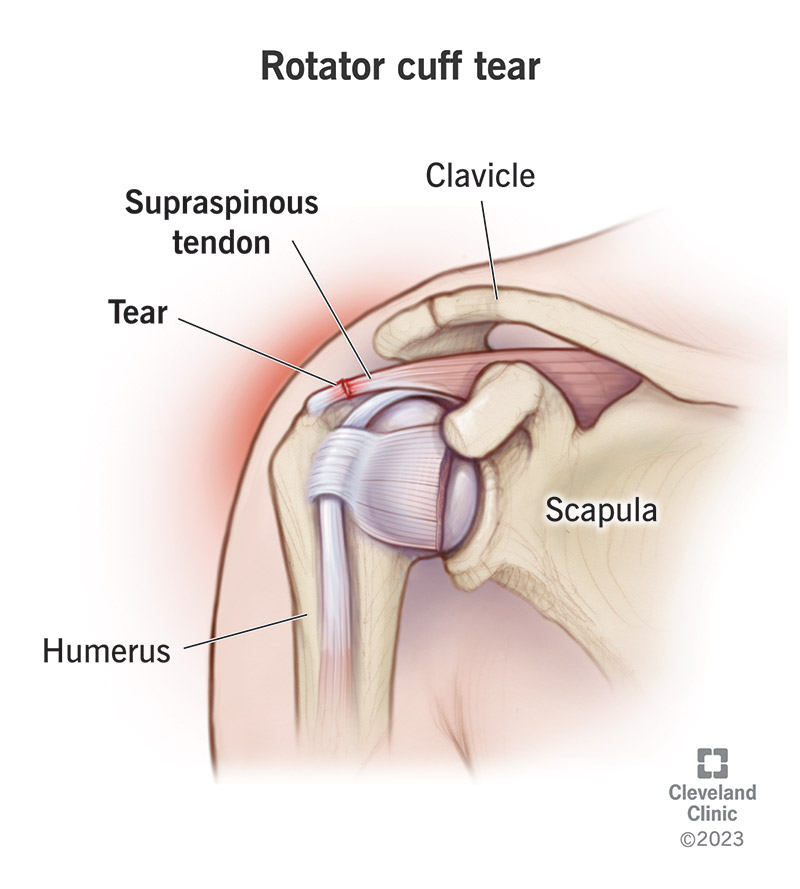
The inability to abduct the arm at the shoulder is a classic sign of a rotator cuff injury. The rotator cuff is responsible for stabilizing the shoulder joint and aiding in various movements, including abduction. When there is a tear or significant weakness in the rotator cuff muscles, especially the supraspinatus muscle, the patient may be unable to lift the arm away from the body or may experience pain while doing so.
Choice B reason:
A negative drop arm test would actually indicate that there is no rotator cuff injury. The drop arm test is performed by asking the patient to fully abduct the arm to 90 degrees and then slowly lower it. If the patient can control the motion and lower the arm smoothly, the test is negative. A positive drop arm test, where the patient cannot control the descent of the arm, would suggest a rotator cuff tear.
Choice C reason:
While an alteration in the contour of the joint may indicate some form of shoulder pathology, it is not specific to a rotator cuff injury. Changes in the contour could be due to various conditions, including dislocation, arthritis, or other musculoskeletal disorders.
Choice D reason:
A positive Tinel's sign is used to diagnose nerve compression or nerve damage, not rotator cuff injuries. It is performed by tapping over the course of a nerve to elicit a tingling sensation or pain in the distribution of the nerve. This sign is commonly associated with conditions like carpal tunnel syndrome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason:
Mucositis is an inflammation of the mucous membranes lining the digestive tract, which is commonly associated with chemotherapy and radiation therapy, not directly with opioid use. While it can be a concern for cancer patients, it is not a typical side effect of opioids.
Choice B reason:
Bleeding is not a common side effect of opioid medications. While cancer patients may experience bleeding due to various reasons, including the cancer itself or treatment-related issues, opioids do not typically cause bleeding.
Choice C reason:
Opioid-induced constipation (OIC) is a common side effect of opioid medications due to their action on the gastrointestinal tract. Opioids reduce gastrointestinal motility, leading to constipation, which can progress to impaction if not managed properly. This is a manifestation that nurses should anticipate and manage proactively in clients taking opioid medications for pain management.
Choice D reason:
Diarrhea is not typically associated with opioid use. In fact, opioids are more likely to cause constipation rather than diarrhea. Diarrhea may occur as a result of other treatments or conditions but is not a direct side effect of opioids.
Correct Answer is D
Explanation
Choice A reason:
Abdominal distention can be a sign of delayed return of peristalsis or ileus, especially when accompanied by other symptoms such as nausea, vomiting, or lack of bowel movement. It is not typically a sign that peristalsis is returning.
Choice B reason:
A request for a cup of tea and some toast may indicate that the client is feeling better and is hungry, which can be a good sign. However, it is not a definitive clinical indicator of the return of peristalsis. The desire to eat does not necessarily mean that the digestive system is ready to process food.
Choice C reason:
Hypoactive bowel sounds in two quadrants may indicate that peristalsis is present but weak. While this could be a sign that peristalsis is starting to return, it is not as strong an indicator as the passage of flatus or stool.
Choice D reason:
The passage of flatus is a clear sign that peristalsis is returning. It indicates that gas is moving through the intestines, which is a function of peristalsis. This is often one of the first signs that the gastrointestinal system is recovering after surgery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today