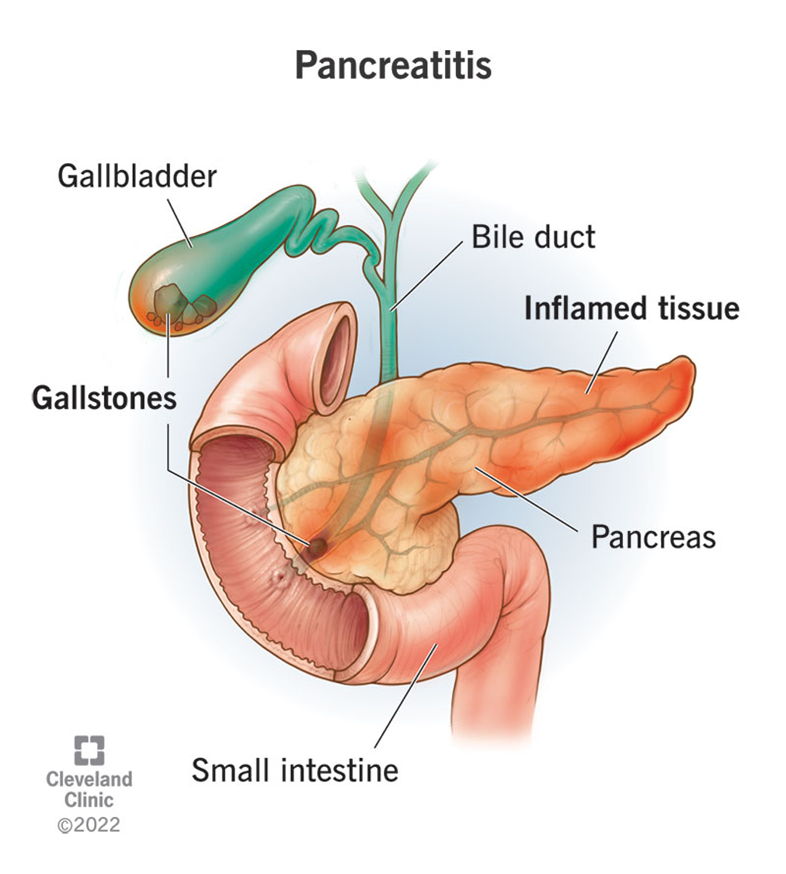
A nurse admits a client to the emergency department who reports nausea and vomiting that worsens when he lies down. Antacids do not help. The provider suspects acute pancreatitis. Which of the following laboratory test results should the nurse expect to see?
Increased serum amylase
Increased serum calcium
Decreased WBC
Decreased serum lipase
The Correct Answer is A
Choice A Reason:
Increased serum amylase is a key indicator of acute pancreatitis. Amylase is an enzyme produced by the pancreas to help digest carbohydrates. In cases of acute pancreatitis, the pancreas becomes inflamed, leading to the release of amylase into the bloodstream. Elevated levels of serum amylase, typically more than three times the upper limit of normal, are a strong indication of acute pancreatitis. This enzyme level usually rises within a few hours of the onset of pancreatitis and can remain elevated for several days.
Choice B Reason:
Increased serum calcium is not typically associated with acute pancreatitis. In fact, acute pancreatitis can often lead to hypocalcemia (low calcium levels) due to fat saponification in the pancreas, where calcium binds with fatty acids. Therefore, an increase in serum calcium would not be expected in a patient with acute pancreatitis. Monitoring calcium levels is important, but an increase is not a diagnostic marker for this condition.
Choice C Reason:
Decreased WBC (white blood cell count) is not a characteristic finding in acute pancreatitis. On the contrary, acute pancreatitis often leads to an elevated WBC count due to the inflammatory response in the body. Leukocytosis (increased WBC) is a common finding in many inflammatory and infectious conditions, including acute pancreatitis. Therefore, a decreased WBC count would not be expected and does not support the diagnosis of acute pancreatitis.
Choice D Reason:
Decreased serum lipase is incorrect. Similar to amylase, lipase is another enzyme produced by the pancreas, which helps in the digestion of fats. In acute pancreatitis, serum lipase levels also increase significantly, often more than three times the upper limit of normal. Lipase levels tend to rise slightly later than amylase but remain elevated for a longer period, making it a useful marker for diagnosing acute pancreatitis. Therefore, decreased serum lipase would not be expected in this condition.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","C","D"]
Explanation
Choice A reason: Monitoring the heart rate is crucial when administering amiodarone, as this drug can cause bradycardia (a slower than normal heart rate). Amiodarone affects the electrical conduction system of the heart, and close monitoring helps ensure that the heart rate remains within a safe range. The normal resting heart rate for adults is typically between 60 and 100 beats per minute.
Choice B reason: Respiratory rate monitoring is essential because amiodarone can cause pulmonary toxicity, which may manifest as interstitial pneumonitis or pulmonary fibrosis. Early detection of respiratory changes can help prevent severe complications. The normal respiratory rate for adults is 12 to 20 breaths per minute.
Choice C reason: Monitoring heart rhythm is necessary because amiodarone is used to treat arrhythmias, and it can also cause new arrhythmias or exacerbate existing ones. Continuous ECG monitoring helps detect any abnormal rhythms early, allowing for prompt intervention. Normal sinus rhythm is characterized by a regular rhythm with a rate of 60 to 100 beats per minute.
Choice D reason: Cardiac output monitoring is important because amiodarone can affect the contractility of the heart and overall cardiac function. Cardiac output is a measure of the amount of blood the heart pumps in one minute, and it is crucial for ensuring adequate tissue perfusion. Normal cardiac output ranges from 4 to 8 liters per minute in adults.
Correct Answer is D
Explanation
Choice A Reason:
Malfunction of the alarm button is unlikely to be the cause of increased peak airway pressure. The alarm is designed to alert the nurse to a problem with the ventilator or the patient’s airway, not to malfunction itself. Therefore, this is not the first thing the nurse should assess.
Choice B Reason:
A cut or slice in the tubing from the ventilator could cause a loss of pressure or air leak, but it would not typically result in increased peak airway pressure. Instead, it would likely cause a decrease in pressure and potentially trigger a different alarm.
Choice C Reason:
Higher than normal endotracheal cuff pressure can contribute to increased peak airway pressure. However, it is not the most immediate concern compared to a kink in the tubing, which can completely obstruct airflow and rapidly compromise the patient’s ventilation.
Choice D Reason:
A kink in the ventilator tubing is a common and immediate cause of increased peak airway pressure. It obstructs the flow of air, leading to a buildup of pressure in the system. This is the first thing the nurse should assess and correct to ensure the patient is receiving adequate ventilation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today