I have edited the text according to your instructions.
text 1:
An older adult with a terminal illness is receiving hospice care and is having difficulty coping with feelings related to death and dying. Which intervention(s) should the nurse include in this client's plan of care? (Select all that apply.)
Instruct client and family to reconsider end of life choices.
Teach client how to use guided imagery.
Record the client's desire to live.
Encourage family to visit frequently.
Encourage family to bring the client old photographs.
Correct Answer : B,C,D,E
Choice A reason: This is incorrect because instructing the client and family to reconsider end of life choices is disrespectful and insensitive. The nurse should respect the client's autonomy and preferences and support their decisions.
Choice B reason: This is correct because teaching the client how to use guided imagery is a helpful intervention for coping with feelings related to death and dying. Guided imagery is a relaxation technique that involves visualizing positive images and scenarios that can reduce stress, anxiety, and pain.
Choice C reason: This is correct because recording the client's desire to live is an important intervention for coping with feelings related to death and dying. The nurse should acknowledge and validate the client's emotions and help them express their hopes and fears.
Choice D reason: This is correct because encouraging family to visit frequently is a beneficial intervention for coping with feelings related to death and dying. The nurse should facilitate family involvement and communication and help the client maintain meaningful relationships.
Choice E reason: This is correct because encouraging family to bring the client old photographs is a useful intervention for coping with feelings related to death and dying. The nurse should assist the client in reminiscing and reviewing their life story and achievements.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Administering a half dose now is not advisable, because it may result in underdosing or overdosing of digoxin. Digoxin has a narrow therapeutic range and a high risk of toxicity, especially in infants and children. The amount of digoxin absorbed by the infant before vomiting is unknown, so giving a partial dose may not achieve therapeutic levels or may exceed safe levels.
Choice B: Giving another dose is not advisable, because it may result in overdosing of digoxin. Digoxin has a narrow therapeutic range and a high risk of toxicity, especially in infants and children. The amount of digoxin absorbed by the infant before vomiting is unknown, so giving a full dose may exceed safe levels and cause adverse effects such as nausea, vomiting, bradycardia, arrhythmias, or visual disturbances.
Choice C: Mixing the next dose with food is not advisable, because it may affect the absorption and bioavailability of digoxin. Digoxin should be taken on an empty stomach or at least one hour before or two hours after meals, because food can interfere with its absorption from the gastrointestinal tract and reduce its effectiveness.
Choice D:Withholding the dose is the safest option. If vomiting occurs within 30 minutes of administration, it’s generally advised to skip that dose to avoid the risk of overdose.The next dose should be given as scheduled Digoxin has a long half-life and accumulates in tissues, so missing one dose will not significantly affect its therapeutic effect. Withholding this dose will avoid overdosing and toxicity of digoxin, which can be life-threatening in infants and children. The nurse should also advise the mother to resume the regular dosing schedule and monitor the infant's pulse rate and signs of digoxin toxicity.
Correct Answer is B
Explanation
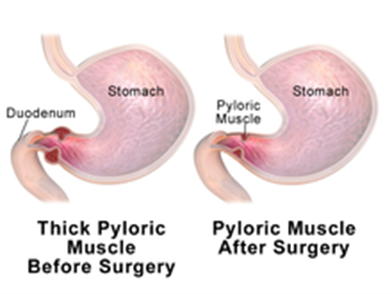
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Choice D reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today