An older client with a history of heart failure and admitted to the medical unit after falling at home and has become increasingly confused. The client's spouse is designated as the client's power of attorney.
When reporting to the healthcare provider using SBAR (Situation, Background, Assessment, Recommendation) communication, which information should the nurse provide first?
Currently prescribed medications.
Fall at home as reason for admission.
Client's healthcare power of attorney.
Increasing confusion of the client.
The Correct Answer is D
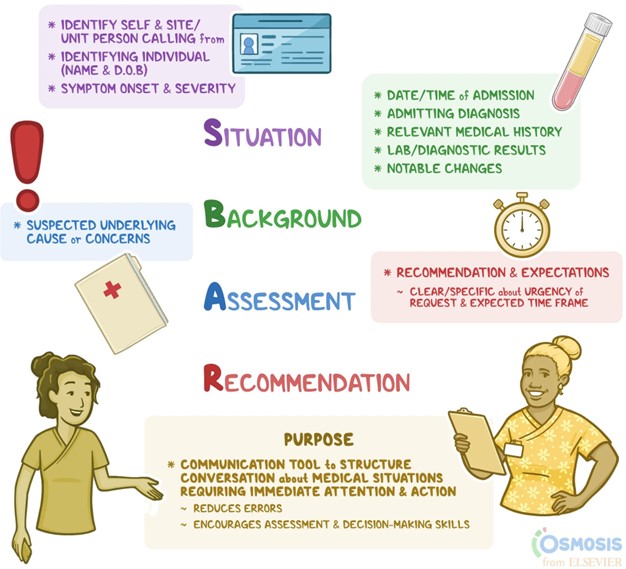
Situation: Increasing confusion of the client.
The nurse should start by providing the current situation, which is the client's increasing confusion. This is crucial information as it indicates a change in the client's condition and may require immediate attention.
Background: Fall at home as reason for admission.
Next, the nurse should provide the background information, which includes the reason for admission, in this case, the fall at home. This helps the healthcare provider understand the context and potential contributing factors to the client's current condition. Assessment: Currently prescribed medications.
After providing the background, the nurse should discuss the assessment findings. In this case, it would be appropriate to mention the client's currently prescribed medications. This information can help the healthcare provider assess for any medication-related issues or interactions that could be contributing to the client's confusion.
Recommendation: Client's healthcare power of attorney.
Lastly, the nurse should provide the recommendation, which in this case is the client's healthcare power of attorney. This information is important as it identifies the designated decision-maker for the client's healthcare decisions and can assist the healthcare provider in involving the appropriate person in the care planning process.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is {"dropdown-group-1":"B","dropdown-group-2":"B"}
Explanation
Correct Answer is ["200"]
Explanation
To calculate the mL/hour for the erythromycin infusion, we first need to determine the infusion rate in mL/minute.
The infusion is to be completed over 30 minutes, which is equal to 0.5 hours. Next, we divide the total volume (100 mL) by the total time (0.5 hours) to get the infusion rate in mL/hour:
Infusion rate = Total volume / Total time
Infusion rate = 100 mL / 0.5 hours Infusion rate = 200 mL/hour
Therefore, the nurse should program the infusion pump to deliver the erythromycin infusion at a rate of 200 mL/hour.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today