A patient is admitted to the hospital with symptoms consistent with a right hemisphere stroke. Which neurovascular assessment requires immediate intervention by the nurse?
Pupillary changes to ipsilateral dilation.
Left-sided facial drooping and dysphagia.
Orientation to person and place only.
Unequal bilateral hand grip strengths.
The Correct Answer is A
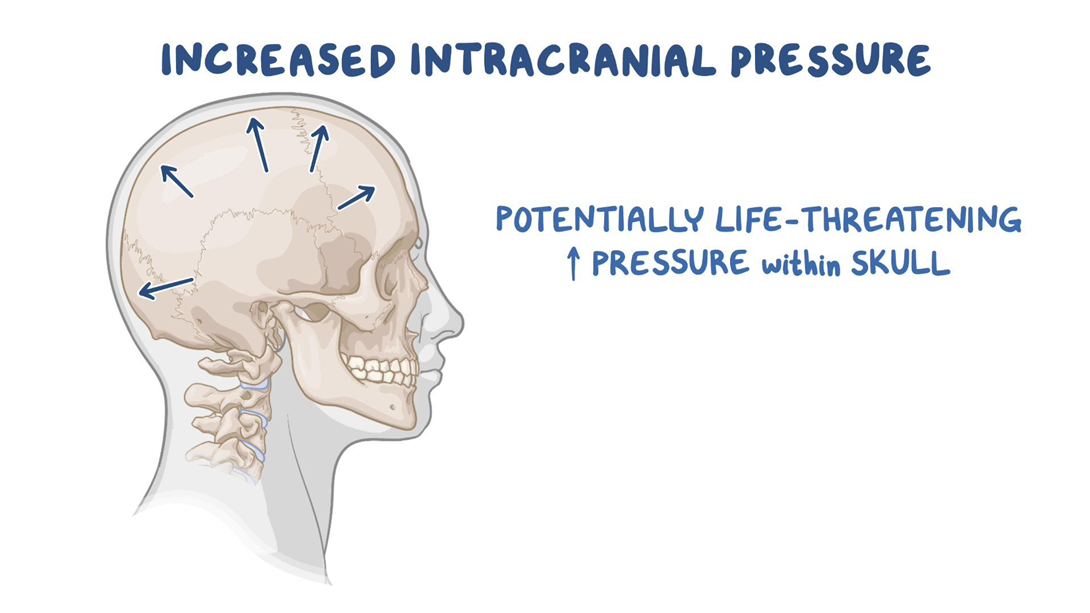
Choice A reason: Pupillary changes to ipsilateral dilation indicate increased intracranial pressure, which is a life-threatening complication of stroke. The nurse should notify the physician and prepare for emergency measures.
Choice B reason: Left-sided facial drooping and dysphagia are common signs of right hemisphere stroke, but they do not require immediate intervention by the nurse. The nurse should monitor the patient's swallowing ability and provide oral care.
Choice C reason: Orientation to person and place only is a sign of impaired cognition, which is also common in right hemisphere stroke. The nurse should assess the patient's memory, judgment, and attention span.
Choice D reason: Unequal bilateral hand grip strengths are a sign of hemiparesis, which is a weakness on one side of the body. The nurse should assist the patient with mobility and prevent contractures.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["F","H"]
Explanation
a) Basic metabolic panel: This is a blood test that measures the levels of electrolytes, glucose, calcium, and kidney function. It is not a priority order for this client because her glucose level is within the normal range and her symptoms are not indicative of electrolyte imbalance or kidney failure.
b) Echocardiogram: This is a test that uses sound waves to create images of the heart and its valves, chambers, and blood flow. It is not a priority order for this client because her chest discomfort may not be related to a cardiac problem and her SpO2 is normal, indicating adequate oxygenation.
c) CT scan of abdomen: This is a test that uses X-rays to create detailed pictures of the organs and structures in the abdomen. It is not a priority order for this client because her abdominal pain is not severe or acute and her nausea and poor appetite may be due to her illness or dialysis.
d) Blood cultures times 2 sets: This is a test that checks for the presence of bacteria or fungi in the blood. It is not a priority order for this client because she does not have signs of infection such as fever, chills, or leukocytosis.
e) Chest X-ray: This is a test that uses X-rays to create images of the lungs and chest wall. It is not a priority order for this client because she does not have respiratory symptoms such as cough, shortness of breath, or wheezes.
f) Place on continuous cardiac monitor: This is an order that requires the nurse to attach electrodes to the client's chest and monitor the heart rate and rhythm continuously. This is a priority order for this client because she has a history of CAD and HTN and reports chest discomfort and lightheadedness, which could indicate a possible myocardial infarction (heart attack) or arrhythmia (irregular heartbeat).
g) CBC: This is a blood test that measures the number and types of blood cells, such as red blood cells, white blood cells, and platelets. It is not a priority order for this client because she does not have signs of anemia, bleeding, or infection.
h) 12 lead EKG: This is a test that records the electrical activity of the heart from 12 different angles. It can detect abnormalities in the heart's rhythm, conduction, or damage. This is a priority order for this client because she has a history of CAD and HTN and reports chest discomfort and lightheadedness, which could indicate a possible myocardial infarction (heart attack) or arrhythmia (irregular heartbeat).
Correct Answer is C
Explanation
Choice A reason: This is incorrect because monitoring pulse oximetry every 2 hours is not a sufficient or timely intervention for the nurse to implement. Pulse oximetry is a noninvasive method of measuring the oxygen saturation of hemoglobin in the blood. Normal oxygen saturation is 95% to 100%, while hypoxemia is less than 90%. However, pulse oximetry may not reflect the severity of respiratory distress or the effectiveness of nebulizer treatment in a client with asthma. Moreover, monitoring pulse oximetry every 2 hours is too infrequent for a client who is in acute respiratory distress and needs more frequent assessment and intervention.
Choice B reason: This is incorrect because teaching proper use of a rescue inhaler is not a priority or relevant intervention for the nurse to implement. A rescue inhaler is a type of short-acting bronchodilator that can be used to relieve acute asthma symptoms by relaxing the smooth muscles of the airways and improving airflow. However, teaching proper use of a rescue inhaler is not an urgent action for a client who is already receiving nebulizer treatment, which delivers a higher dose of medication directly to the lungs. Moreover, teaching proper use of a rescue inhaler is not appropriate for a client who is in respiratory distress and may not be able to focus or retain information.
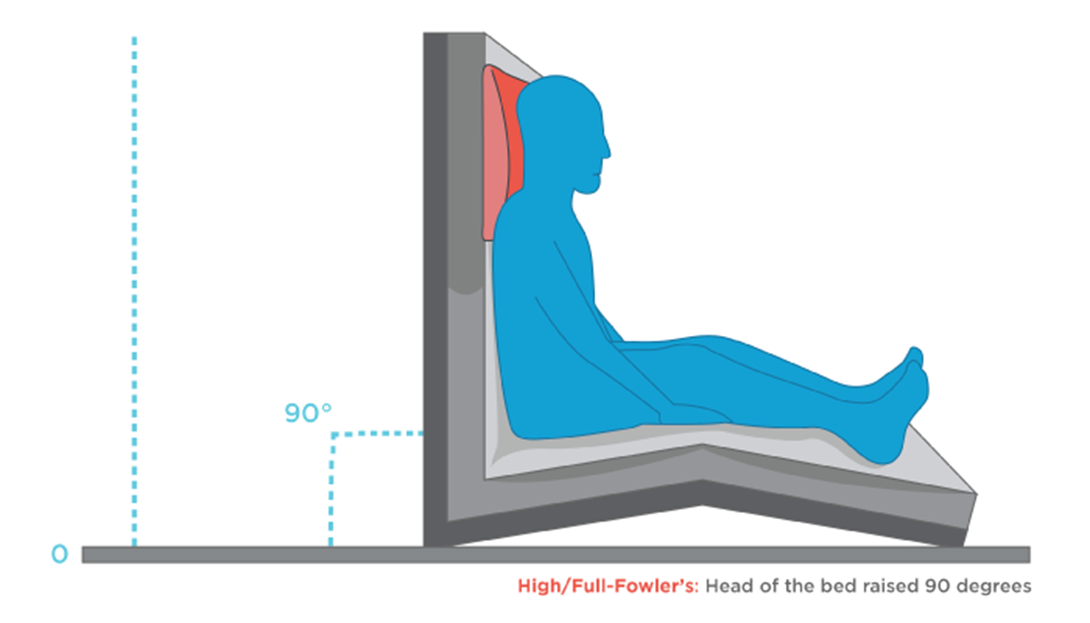
Choice C reason: This is correct because elevating the head of bed to 90 degrees is the most important intervention for the nurse to implement. Elevating the head of bed to 90 degrees can help improve breathing and oxygenation by reducing pressure on the diaphragm and chest wall, increasing lung expansion and ventilation, and facilitating expectoration of mucus. This can enhance the effects of nebulizer treatment and reduce respiratory distress in a client with asthma.
Choice D reason: This is incorrect because determining exposure to asthmatic triggers is not an immediate or helpful intervention for the nurse to implement. Asthmatic triggers are substances or factors that can cause or worsen asthma symptoms by inducing inflammation or constriction of the airways. Examples of asthmatic triggers include allergens, irritants, infections, exercise, stress, or weather changes. However, determining exposure to asthmatic triggers is not a priority action for a client who is in respiratory distress and needs more urgent interventions to improve breathing and oxygenation. Moreover, determining exposure to asthmatic triggers may not change the management or outcome of an acute asthma attack that has already occurred.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today