A nurse working on a medical-surgical unit is notified about a mass casualty event that recently took place in the community.
Which of the following assignments should the nurse anticipate?
Assist in discharging stable clients to home.
Determine the acuity and number of casualties arriving at the facility.
Delegate tasks to emergency health care specialists.
Provide informational updates to members of the media.
The Correct Answer is B
Choice A rationale:
Assisting in discharging stable clients to home is not the most appropriate assignment when a mass casualty event has occurred. During such events, resources are needed for critically injured patients, and stable clients can typically be discharged by non-emergency staff.
Choice B rationale:
Determining the acuity and number of casualties arriving at the facility is the most appropriate assignment during a mass casualty event. This information is critical for allocating resources and providing the necessary level of care to those affected.
Choice C rationale:
Delegating tasks to emergency healthcare specialists may be necessary, but it is not the initial assignment for the nurse working on a medical-surgical unit. Assessing the situation and determining the acuity of incoming casualties take precedence.
Choice D rationale:
Providing informational updates to members of the media is not the role of a nurse during a mass casualty event. This task should be handled by hospital public relations or designated spokespersons to ensure accurate and controlled information dissemination.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
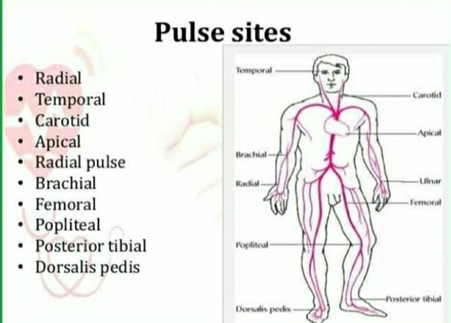
- A radial pulse is the pulse felt at the wrist, where the radial artery runs along the thumb side of the forearm. It is one of the most common sites for measuring a person's heart rate.
- To measure a radial pulse, the examiner should place two or three fingers over the radial artery, just below the wrist crease, and apply gentle pressure until a pulsation is felt. The examiner should not use the thumb, as it has its own pulse and may interfere with the accuracy of the measurement. The examiner should count the number of beats for 15, 30, or 60 seconds, depending on the regularity and rate of the pulse.
- In the picture, the unlicensed assistive personnel (UAP) is using the thumb to measure the radial pulse, which is incorrect. The practical nurse (PN) should demonstrate the correct pulse site to the UAP and explain why using the thumb is not appropriate. This will help to ensure that the UAP obtains an accurate and reliable pulse rate for the client.
Therefore, option C is the correct answer, while options A, B, and D are incorrect.
Option A is incorrect because instructing the UAP to report any abnormal findings does not address the error in technique.
Option B is incorrect because reminding the UAP to check the pulse volume does not address the error in technique.
Option D is incorrect because confirming the accuracy of the pulse rate obtained by the UAP does not address the error in technique.
Correct Answer is B
Explanation
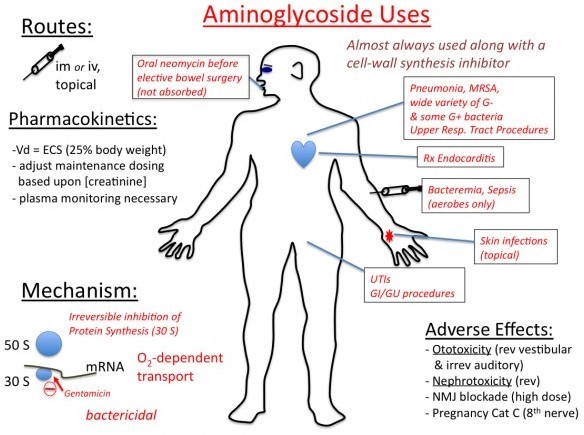
This is the correct answer because it is the best way to assess for signs of ototoxicity, which is a potential adverse effect of aminoglycosides. Ototoxicity is the damage or injury to the inner ear or auditory nerve caused by certain drugs or chemicals. It can result in hearing loss, tinnitus, vertigo, or balance problems. Aminoglycosides are a class of antibiotics that are effective against gram-negative bacteria, but they can also cause ototoxicity by interfering with the function of the hair cells in the cochlea. The practical nurse (PN) should monitor the client's hearing by asking about any changes in hearing acuity, ringing in the ears, or difficulty understanding speech. The PN should also perform a hearing test using a tuning fork or an audiometer if available. The PN should report any signs of ototoxicity to the health care provider and discontinue the aminoglycoside as ordered.
a) Check for changes in vision.
This is not the correct answer because it is not related to ototoxicity. Vision is the ability to see and perceive objects and colors using the eyes and the brain. Vision may be affected by various factors, such as age, genetics, eye diseases, injuries, infections, or medications. However, aminoglycosides do not cause vision problems or impairments. The PN should check for changes in vision in a client who is receiving other drugs that can cause ocular toxicity, such as ethambutol, chloroquine, or digoxin.
c) Observe the skin for a rash.
This is not the correct answer because it is not related to ototoxicity. A rash is a change in the color, texture, or appearance of the skin that may be caused by various factors, such as allergies, infections, inflammation, or medications. A rash may present as redness, itching, swelling, blisters, bumps, or scales.
Aminoglycosides can cause skin reactions such as rash or urticaria in some clients who are hypersensitive or allergic to them. The PN should observe the skin for a rash in a client who is receiving an aminoglycoside and report any signs of an allergic reaction to the health care provider. However, a rash is not a sign of ototoxicity.
d) Measure the urinary output.
This is not the correct answer because it is not related to ototoxicity. Urinary output is the amount of urine produced and excreted by the kidneys and bladder. It is an indicator of renal function and fluid balance. The normal range for urinary output is 0.5 to 1 mL/kg/hour for adults. Urinary output may be affected by various factors, such as fluid intake, dehydration, diuretics, kidney disease, or medications. Aminoglycosides can cause nephrotoxicity, which is another potential adverse effect of these drugs. Nephrotoxicity is the damage or injury to the kidneys caused by certain drugs or chemicals. It can impair the kidneys' ability to filter waste products from the blood, resulting in reduced urine production and oliguria. The PN should measure the urinary output in a client who is receiving an aminoglycoside and report any signs of nephrotoxicity to the health care provider. However, urinary output is not a sign of ototoxicity
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today