A nurse reinforcing teaching about vitamin K with a client who is postpartum. Which of the following statements should the nurse include?
Vitamin K decreases the newborn's risk of jaundice.
Vitamin K decreases the newborn's risk of health care-associated infections.
Vitamin K decreases the newborn's risk of hemorrhagic disorders.
Vitamin K decreases the newborn's risk of complications from the Hepatitis B vaccine.
The Correct Answer is C
Choice A rationale :
Vitamin K decreases the newborn's risk of jaundice. Rationale: This statement is incorrect. Vitamin K plays no direct role in reducing the risk of jaundice in newborns. Jaundice is primarily caused by the accumulation of bilirubin in the blood, which is a different issue than hemorrhagic disorders.
Choice B rationale
Vitamin K decreases the newborn's risk of healthcare-associated infections. Rationale: This statement is incorrect. Vitamin K is not related to reducing the risk of healthcare-associated infections. Its main function is related to blood clotting and preventing hemorrhagic disorders.
Choice C rationale
Vitamin K decreases the newborn's risk of hemorrhagic disorders. Rationale: This statement is correct. Vitamin K is essential for the production of clotting factors in the blood, which helps prevent bleeding or hemorrhagic disorders in newborns. Newborns are born with low levels of vitamin K, so administering a vitamin K injection at birth is a common practice to prevent potential bleeding issues.
Choice D rationale
Vitamin K decreases the newborn's risk of complications from the Hepatitis B vaccine. Rationale: This statement is incorrect. Vitamin K is not directly related to reducing the risk of complications from the Hepatitis B vaccine. The vaccine is designed to protect against Hepatitis B infection, and vitamin K is not involved in its efficacy or safety.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice D rationale:
The nurse should state, "The purpose of this medication is to boost fetal lung maturity.”. The rationale behind this choice is that betamethasone is a corticosteroid medication commonly administered to women at risk of preterm delivery between 24 and 34 weeks of gestation. Its primary goal is to accelerate fetal lung maturation by promoting the production of surfactant, a substance that coats the lungs and prevents their collapse. By enhancing lung development, the medication helps reduce the risk of respiratory distress syndrome and other respiratory complications that premature infants might face. It does not directly impact fetal heart rate (Choice A), halt cervical dilation (Choice B), or stop preterm labor contractions (Choice C).
Choice A rationale:
The nurse should not state, "The purpose of this medication is to increase the fetal heart rate.”. Betamethasone does not affect the fetal heart rate, as it is primarily used to enhance lung maturity, as mentioned earlier. The incorrect statement may lead to confusion and misunderstanding of the medication's intended purpose.
Choice B rationale:
The nurse should not state, "The purpose of this medication is to halt cervical dilation.”. Betamethasone does not stop or halt cervical dilation. Its main action is on the fetal lungs to promote surfactant production. Cervical dilation is a natural process that occurs during labor and is not influenced by this medication.
Choice C rationale:
The nurse should not state, "The purpose of this medication is to stop preterm labor contractions.”. Betamethasone is not used to stop or prevent preterm labor contractions directly. Instead, its focus is on improving fetal lung maturity to enhance the baby's respiratory function once born prematurely.
Correct Answer is A
Explanation
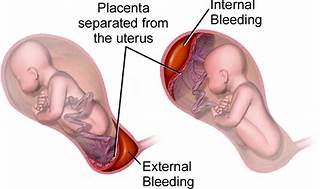
The correct answer is choice A, Maternal hypertension.
Choice A rationale:
Maternal hypertension is widely recognized as the most common risk factor for placental abruption. High blood pressure can cause the placenta to detach from the uterine wall, leading to abruption. In summary, while all the listed factors can contribute to the risk of placental abruption, maternal hypertension stands out as the most common cause, supported by multiple health sources. It’s important for nurses to recognize and manage hypertension in pregnant clients to minimize the risk of this serious complication.
Choice B rationale:
While maternal cocaine use is a significant risk factor for placental abruption due to its vasoconstrictive effects, which can compromise the placental blood flow, it is not as common as maternal hypertension.
Choice C rationale:
Maternal cigarette smoking is also a risk factor for placental abruption. Smoking can lead to a variety of complications in pregnancy, including placental problems, but again, it is less common than hypertension as a cause for abruption.
Choice D rationale:
Maternal battering can lead to trauma which may result in placental abruption. However, it is not considered the most common risk factor when compared to maternal hypertension.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today