A nurse is teaching a client who has schizophrenia a new prescription for lurasidone. Which of the following information should the nurse include in the teaching?(Select all that apply.).
Take this medication on an empty stomach.
Avoid drinking grapefruit juice while taking this medication.
Change positions slowly while taking this medication.
This medication can cause insomnia.
It is possible to experience involuntary movements while taking this medication.
Correct Answer : B,D
Choice A rationale:
Lurasidone does not necessarily need to be taken on an empty stomach. It can be taken with or without food.
Choice B rationale:
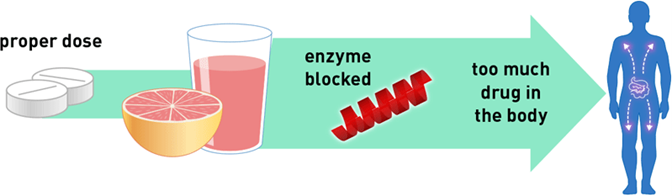
Avoiding grapefruit juice is essential with lurasidone as it can interfere with the drug's metabolism and increase the risk of side effects.
Choice C rationale:
Changing positions slowly is relevant for medications that can cause orthostatic hypotension, but lurasidone is not typically associated with this side effect.
Choice D rationale:
Lurasidone can cause insomnia in some individuals, so it is important for the client to be aware of this potential side effect. It is best taken in the evening to minimize this effect.
Choice E rationale:
While involuntary movements (extrapyramidal symptoms) can occur with some antipsychotic medications, lurasidone has a lower risk of causing these side effects compared to older antipsychotics. It is not a major concern with lurasidone treatment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Answer: A. Diplopia.
Rationale:
A) Diplopia: Diplopia, or double vision, is a common symptom in multiple sclerosis (MS) due to demyelination of nerves in the brainstem, affecting eye movement coordination. This visual disturbance is frequently seen in MS clients and may worsen during flare-ups.
B) Masklike expression: A masklike expression is more commonly associated with Parkinson’s disease rather than multiple sclerosis. This characteristic facial appearance is due to muscle rigidity, which is not typically a manifestation of MS.
C) Twitching of the face: Facial twitching, or fasciculations, is not typically a primary symptom of multiple sclerosis. While muscle weakness and spasticity are common in MS, twitching is more commonly seen in conditions such as amyotrophic lateral sclerosis (ALS).
D) Agitation: Agitation is not a primary symptom of MS. While MS can lead to cognitive changes or mood disturbances, such as depression, severe agitation is more commonly linked with other neurological or psychiatric conditions.
Correct Answer is B
Explanation
Choice A rationale:
Is not a safe fall prevention strategy. Securing cords under carpeting can create tripping hazards. It is better to keep cords away from commonly used walking paths or use cord covers to prevent falls.
Choice B rationale:
Purchasing a skid-proof bathtub mat is a good fall-prevention strategy for an older adult client. It helps prevent slipping and falling in the bathroom, which is a common area for accidents in older adults.
Choice C rationale:
Is not a recommended fall prevention strategy. Leather soles can be slippery on smooth surfaces, increasing the risk of falls. Instead, the client should wear shoes with rubber soles that provide better traction.
Choice D rationale:
Is not the best option. Throw rugs, even with rubber backing, can still shift or bunch up, posing a tripping hazard. It's safer to avoid using throw rugs altogether or ensure they are firmly secured to the floor.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today