A nurse is providing care for an older adult client who has diabetes insipidus (DI). The nurse should monitor the client for which of the following neurological effects?
Hypotension
Poor skin turgor
Ataxia
Dilute urine
The Correct Answer is C
Choice A reason: Hypotension
Hypotension, or low blood pressure, can be a consequence of dehydration, which is a common complication of DI due to the excessive loss of water. However, hypotension is not a direct neurological effect of DI. It is more of a circulatory system response to the changes in fluid volume within the body.
Choice B reason: Poor skin turgor
Poor skin turgor is an indicator of dehydration, which can occur in DI due to the large volume of urine excreted. Skin turgor refers to the skin's ability to change shape and return to normal (elasticity), and it becomes less elastic when the body is dehydrated. While this is an important sign to monitor, it is not a neurological effect.
Choice C reason: Ataxia
Ataxia, which is a lack of muscle coordination affecting speech, eye movements, the ability to swallow, walking, picking up objects, and other voluntary movements, can be a neurological effect of DI if severe dehydration and electrolyte imbalance affect the brain. Symptoms such as confusion and muscle cramps can also be associated with ataxia, making it a relevant neurological effect to monitor in a client with DI.
Choice D reason: Dilute urine
Dilute urine is a primary symptom of DI, not a neurological effect. It is the result of the kidneys' inability to concentrate urine due to a deficiency in the anti-diuretic hormone (ADH) or the kidneys' response to ADH. Monitoring urine concentration is crucial in managing DI, but it does not represent a neurological effect.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason:
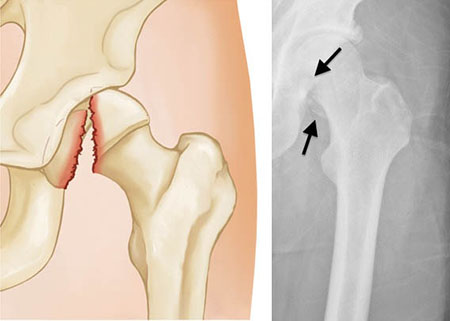
Pneumothorax, a collapsed lung, can indeed cause shortness of breath and dyspnea. However, it is typically associated with a sudden onset of these symptoms following a chest injury or spontaneously in the case of a ruptured air blister. In the context of a femoral head fracture, pneumothorax is less likely unless there was additional trauma to the chest area.
Choice B reason:
Pneumonia is an infection of the lungs that leads to inflammation of the air sacs, causing them to fill with fluid or pus. Symptoms include cough with phlegm, fever, chills, and difficulty breathing. While pneumonia could cause dyspnea, it usually develops due to an infectious process rather than directly from a femoral head fracture.
Choice C reason:
Airway obstruction involves a blockage that prevents air from passing freely to the lungs. It can be caused by foreign objects, swelling due to allergic reactions, or other medical conditions. The symptoms of airway obstruction include difficulty breathing, wheezing, and potential changes in skin color. However, airway obstruction is not commonly a direct complication of a femoral head fracture.
Choice D reason:
Fat embolism syndrome is a serious condition that occurs when fat globules enter the bloodstream and lodge within the pulmonary vasculature, leading to respiratory distress. It is a known complication following long bone fractures, such as the femur, and presents with symptoms like shortness of breath, hypoxemia, and neurological manifestations. Given the recent femoral head fracture and the symptoms reported, fat embolism syndrome is the most likely diagnosis.
Correct Answer is C
Explanation
Choice A reason:
While explaining discharge instructions is an important part of patient education and ensuring safety after leaving the hospital, it is not the immediate priority. The nurse must first address any potential medical issues that could compromise the patient's health, such as circulation and nerve function in the affected limb.
Choice B reason:
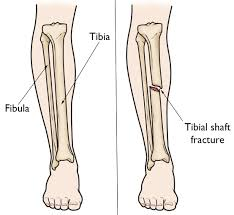
Applying an ice pack to the casted leg can help reduce swelling and provide comfort to the client. This is often recommended for the first 24 to 72 hours after the cast is applied, especially if the cast is on a leg. However, this is secondary to assessing the neurovascular status of the limb.
Choice C reason:
Performing a neurovascular assessment is the priority action for the nurse. This assessment includes checking for sensation, warmth, capillary refill, pulses, and movement. It is crucial to identify any signs of compromised blood flow or nerve injury early to prevent further complications.
Choice D reason:
Providing reassurance to the client and parents is important for emotional support and can help alleviate anxiety. However, the nurse's immediate priority is to ensure the physical well-being of the client, which includes performing a neurovascular assessment to detect any urgent issues.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today