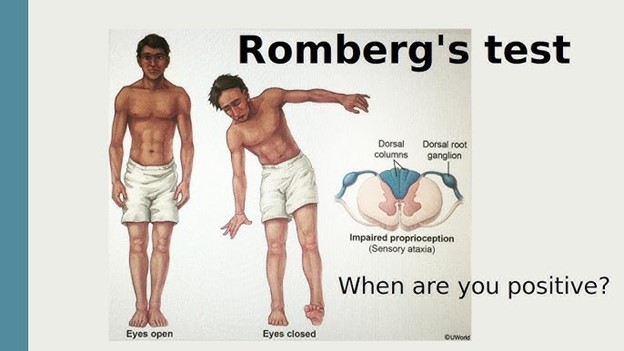
A nurse is preparing a client for a Romberg test. Which of the following statements should the nurse make?
"Stand with your feet together and your arms at your sides.”
"After I place the tuning fork, tell me when you no longer hear the sound.”
"I'm going to stroke the lateral side of the bottom of your foot.”
"Touch each fingertip as quickly as possible with your thumb.”
The Correct Answer is A
The correct answer is choice A: "Stand with your feet together and your arms at your sides."
Choice A rationale:
This statement is correct. The nurse should instruct the client to stand with their feet together and their arms at their sides for a Romberg test. This position helps to assess the client's ability to maintain balance with minimal sensory input, evaluating their proprioception and vestibular function.
Choice B rationale:
The instruction about the tuning fork is unrelated to the Romberg test. The tuning fork is commonly used to assess hearing and vibratory sensations, not balance.
Choice C rationale:
This statement is unrelated to the Romberg test. Mentioning the lateral side of the foot suggests a neurological examination related to assessing reflexes, such as the Babinski reflex.
Choice D rationale:
This instruction pertains to a different test known as the "finger-to-nose" test, which is used to assess coordination, not balance.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The correct answer is Choice C: "Do you consume pork products?"
Choice C rationale: Islamic dietary laws, also known as Halal, prohibit the consumption of pork and its by-products. By asking the client about their consumption of pork products, the nurse demonstrates cultural sensitivity and ensures that the client's dietary preferences and religious practices are respected while under the facility's care.
Choice A rationale: Asking the client if they receive Holy Communion is not appropriate, as this practice is associated with Christianity rather than Islam. This question does not effectively address the client's religious preferences or needs in relation to their Islamic faith.
Choice B rationale: Inquiring about adherence to a kosher diet is not relevant, as this dietary practice is specific to Judaism and does not pertain to the Islamic faith. The nurse should be aware of the distinctions between religious practices when providing culturally competent care.
Choice D rationale: There is no general prohibition against blood transfusions in Islam. Islamic teachings generally permit medical treatments, including blood transfusions, when deemed necessary for the well-being and preservation of life. Asking the client about opposition to blood transfusions would not be the most effective way to clarify their religious preferences in the context of Islam.
Correct Answer is D
Explanation
The correct answer is choice d. Notify the charge nurse of the client’s concerns.
Choice A rationale:
Offering information about alternative therapies is not appropriate in this situation. The nurse’s role is to ensure the client understands the current procedure and to address their concerns, not to suggest alternatives unless directed by the healthcare provider.
Choice B rationale:
Contacting a family member to convince the client to change their mind is not ethical. The decision to proceed with surgery should be made by the client, based on their understanding and consent, not under pressure from family members.
Choice C rationale:
Telling the client the benefits of the surgery might be helpful, but it does not address the client’s lack of understanding about the procedure. The nurse should ensure the client has all the necessary information to make an informed decision.
Choice D rationale:
Notifying the charge nurse of the client’s concerns is the correct action. The charge nurse can facilitate further discussion with the surgeon to ensure the client receives the necessary information and support to make an informed decision. This ensures that the client’s autonomy and right to informed consent are respected.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today