A nurse is performing a cranial nerve assessment on a client following a head injury. Which of the following findings should the nurse expect if the client has impaired function of the vestibulocochlear nerve (cranial nerve VIII)?
Inability to smell
Loss of peripheral vision
Disequilibrium with movement
Deviation of the tongue from midline
The Correct Answer is C
C. The vestibulocochlear nerve is responsible for both the vestibular function and the cochlear function. Impaired function of the vestibulocochlear nerve could result in symptoms related to vestibular dysfunction, such as disequilibrium (feeling unsteady or off balance) especially with movement.
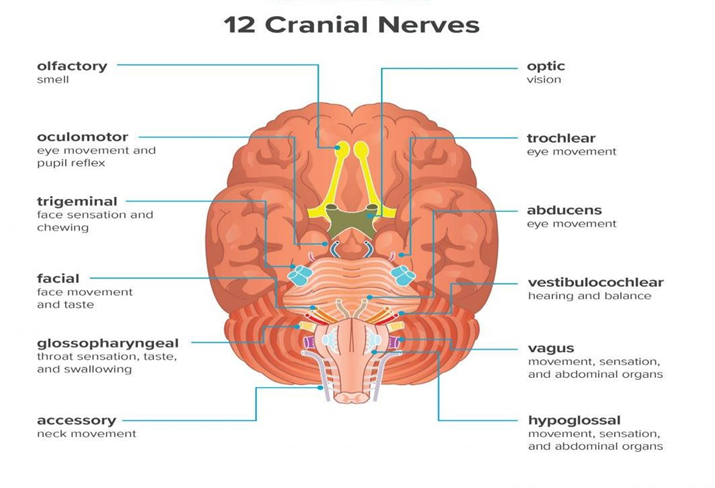
A. The olfactory nerve (cranial nerve I) is responsible for the sense of smell.
B. Loss of peripheral vision is typically associated with impairment of the optic nerve (cranial nerve II), which is responsible for vision.
D. Deviation of the tongue occurs in injury to the hypoglossal nerve.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
D. Extreme temperatures, both hot and cold, can trigger sickle cell crises in individuals with sickle cell disease. Cold temperatures can cause vasoconstriction and increase the risk of sickling of red blood cells, while hot temperatures can lead to dehydration. Therefore, clients with sickle cell disease should avoid exposure to extreme temperatures and take precautions to maintain a comfortable environment, especially during hot summer months and cold winter seasons.
A. Clients with sickle cell disease are at increased risk of developing complications from influenza (flu) infections. Therefore, it is highly recommended that clients with sickle cell disease receive an annual flu vaccination to reduce their risk of contracting the flu and its associated complications.
B. Hydration is crucial for individuals with sickle cell disease as it helps prevent dehydration and reduces the risk of sickling of red blood cells, which can trigger a sickle cell crisis.
C. Alcohol can exacerbate dehydration and increase the risk of vaso-occlusive crises in individuals with sickle cell disease.
Correct Answer is D
Explanation
D. Diet plays a crucial role in managing ulcerative colitis symptoms. Certain foods may trigger flare-ups, while others may be better tolerated. A dietitian can provide personalized dietary advice to help manage symptoms, ensure adequate nutrition, and optimize overall health.
A. Ulcerative colitis is a chronic inflammatory bowel disease that primarily affects the colon and rectum. While pain management is crucial, it is not a priority at this point.
B. Hospice services are generally provided to individuals who have a terminal illness and are nearing the end of life. While ulcerative colitis can be a serious condition, it is not typically considered a terminal illness in itself.
C. A wound, ostomy, and continence nurse (WOCN) specializes in the care of patients with ostomies (such as those resulting from surgery for ulcerative colitis), wounds, and continence issues. The client does not require the services at this point as the decision for the surgery has not been made.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today