A nurse is giving a change-of-shift report using SBAR to the oncoming nurse on a client who has a traumatic brain injury. Which of the following information should the nurse include in the background segment of SBAR?
Plan of care changes for the upcoming shift
Intracranial pressure readings
Glasgow results
Code status
The Correct Answer is D
Choice A reason: Plan of care changes for the upcoming shift
Plan of care changes for the upcoming shift are typically included in the “Recommendation” segment of SBAR. This section focuses on what actions need to be taken next, including any changes in the care plan that the oncoming nurse should be aware of. It ensures that the incoming nurse knows what to expect and what specific tasks or interventions are required during their shift.
Choice B reason: Intracranial pressure readings
Intracranial pressure (ICP) readings are crucial for monitoring a client with a traumatic brain injury. However, these readings are more appropriately included in the “Assessment” segment of SBAR. The assessment section provides an analysis of the client’s current condition, including vital signs, lab results, and other critical data. This information helps the oncoming nurse understand the client’s current status and any immediate concerns.
Choice C reason: Glasgow results
The Glasgow Coma Scale (GCS) results are used to assess the level of consciousness in clients with brain injuries. These results should also be included in the “Assessment” segment of SBAR. The GCS score provides valuable information about the client’s neurological status and helps guide clinical decisions. Including this information in the assessment ensures that the oncoming nurse has a clear understanding of the client’s current condition.
Choice D reason: Code status
Code status is a critical piece of information that should be included in the “Background” segment of SBAR. The background section provides relevant clinical history and context for the current situation. Knowing the client’s code status (e.g., full code, do not resuscitate) is essential for making informed decisions about their care, especially in emergency situations. Including this information in the background ensures that the oncoming nurse is aware of the client’s preferences and legal directives.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Dependent rubor
Dependent rubor is a reddish discoloration of the skin that occurs when the leg is in a dependent position (hanging down). This condition is typically associated with arterial insufficiency rather than chronic venous insufficiency. Arterial insufficiency occurs when there is inadequate blood flow through the arteries, leading to symptoms such as pain, cramping, and changes in skin color. Dependent rubor is a sign of poor arterial circulation and is not commonly seen in venous insufficiency.
Choice B reason: Thick, deformed toenails
Thick, deformed toenails can be a sign of fungal infections or other conditions affecting the nails, but they are not specifically indicative of chronic venous insufficiency. While individuals with chronic venous insufficiency may have poor circulation that can contribute to nail problems, this symptom is not a primary or common finding associated with the condition. Instead, it is more often related to other underlying health issues.
Choice C reason: Hair loss
Hair loss on the legs can occur due to various reasons, including poor circulation. However, it is more commonly associated with arterial insufficiency rather than chronic venous insufficiency. In arterial insufficiency, the reduced blood flow can lead to hair loss, shiny skin, and other changes in the lower extremities. Chronic venous insufficiency primarily affects the veins and leads to symptoms such as swelling, varicose veins, and skin changes.
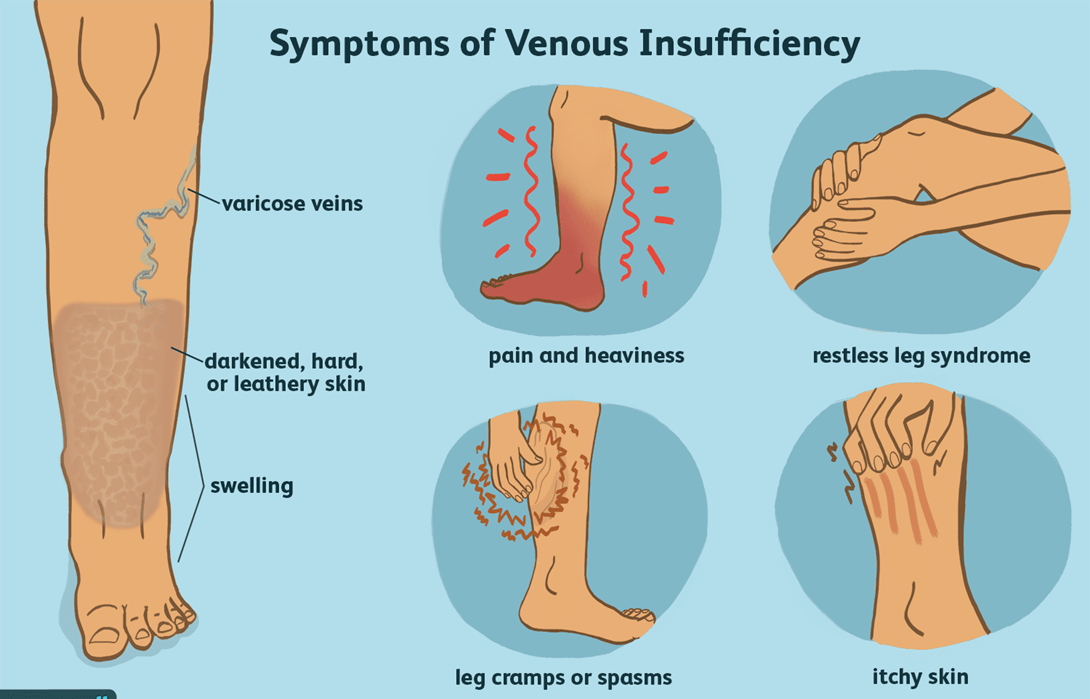
Choice D reason: Edema
Edema, or swelling, is a hallmark symptom of chronic venous insufficiency. This condition occurs when the veins in the legs are unable to effectively return blood to the heart, leading to blood pooling in the lower extremities. The increased pressure in the veins causes fluid to leak into the surrounding tissues, resulting in swelling. Edema is often more pronounced at the end of the day or after prolonged periods of standing or sitting. Managing edema is a key aspect of treating chronic venous insufficiency, and it often involves the use of compression stockings, elevation of the legs, and other measures to improve venous return.
Correct Answer is B
Explanation
Choice A reason:
Health care provider: While health care providers, such as doctors, have extensive knowledge about medications and their uses, they may not always have the most up-to-date information on specific drug compatibilities. Pharmacists specialize in medications and are more likely to have immediate access to detailed compatibility data.
Choice B reason:
Hospital pharmacist: Pharmacists are the primary resource for information on drug compatibility. They have access to comprehensive databases and resources that provide detailed information on drug interactions and compatibility. Consulting the hospital pharmacist ensures that the nurse receives accurate and current information regarding the safe administration of ampicillin and gentamicin sulfate.
Choice C reason:
Nurse manager: Nurse managers oversee nursing staff and ensure that patient care standards are met. While they have a broad knowledge of clinical practices, they may not have the specific expertise or resources to provide detailed information on drug compatibility.
Choice D reason:
Medication sales representative: Medication sales representatives are knowledgeable about the products they promote, but their primary role is to market medications. They may not have the comprehensive and unbiased information needed to determine drug compatibility. It is always best to consult a pharmacist for this type of information.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today