A nurse is creating an education plan for a client who has diverticulosis. The nurse should plan to include which of the following in the client education?
Increase protein from red meat
Decrease fluid intake
Incorporate soft foods that are pureed in consistency
Increase dietary fiber
The Correct Answer is D
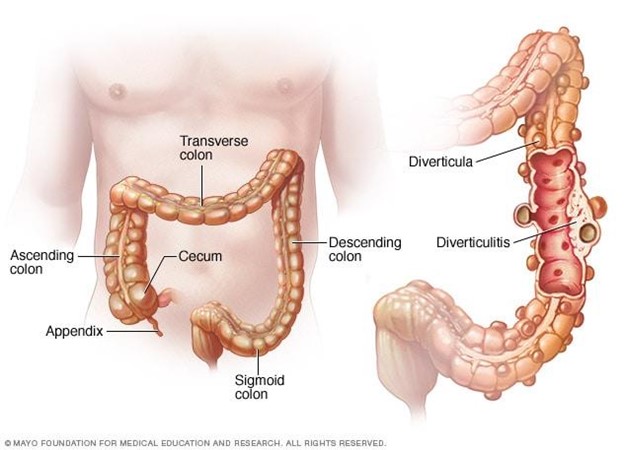
Choice A Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
Choice B Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
Choice C Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
Choice D Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This choice is incorrect. Inability to perform within normal limits is a vague and general term that does not describe the specific finding of left facial droop. The nurse should document the exact observation and compare it to the expected or normal range.
Choice B Reason: This choice is incorrect. Symmetrical findings mean that both sides of the body or face are equal or similar in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is not symmetrical.
Choice C Reason: This is the correct choice. Asymmetrical findings mean that both sides of the body or face are unequal or different in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is asymmetrical.
Choice D Reason: This choice is incorrect. Bilateral strength present means that both sides of the body or face have normal or adequate muscle power or force. Left facial droop indicates that one side of the face has reduced or impaired muscle power or force, which is not bilateral strength present.
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because a referral to a sleep study program is not the most appropriate plan of care for a blind client who has difficulty with sleep. A sleep study program is used to diagnose and treat sleep disorders such as sleep apnea, narcolepsy, or restless legs syndrome.
Choice B Reason: This is incorrect because assisting the client to see if a night shift job is available is not a helpful plan of care for a blind client who has difficulty with sleep. A night shift job can disrupt the circadian rhythm and worsen the sleep quality and quantity of the client.
Choice C Reason: This is incorrect because institution of opioids and sedatives is not a safe plan of care for a blind client who has difficulty with sleep. Opioids and sedatives can cause addiction, dependence, tolerance, and withdrawal symptoms. They can also impair the respiratory and cognitive functions of the client.
Choice D Reason: This is the correct choice because education about non-24 disorder is an essential plan of care for a blind client who has difficulty with sleep. Non-24 disorder is a condition where the internal clock of the body does not synchronize with the 24-hour day-night cycle. It can cause irregular sleep patterns, daytime fatigue, and mood disturbances. It is more common in blind people who lack light perception. The nurse should educate the client about the causes, symptoms, and treatments of non-24 disorder.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today