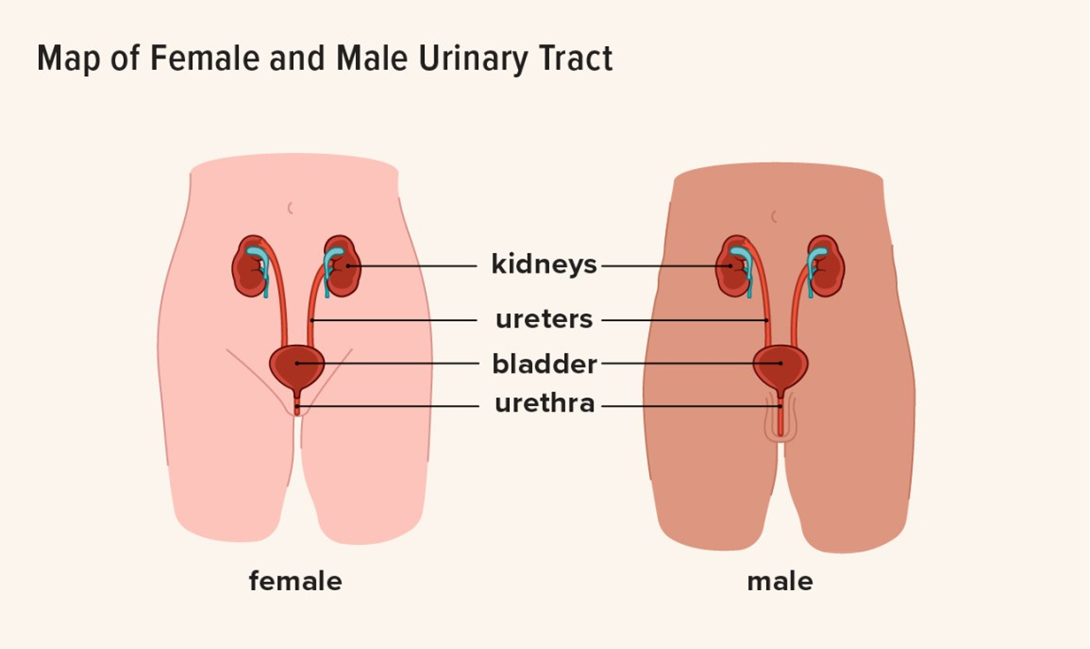
A nurse is collecting data on an older adult client. Which of the following findings should indicate to the nurse that the client has a bladder infection?
Changed mental status
WBC count 9,000/mm³
Diminished reflexes
Temperature 37.3°C (99.1°F)
The Correct Answer is A
Choice A reason: Changed mental status, such as confusion, agitation, or delirium, can be a sign of a bladder infection in older adults, as they may not have the typical symptoms of dysuria, frequency, or urgency.
Choice B reason: WBC count 9,000/mm³ is within the normal range of 4,500 to 11,000/mm³ and does not indicate an infection.
Choice C reason: Diminished reflexes are not related to a bladder infection and may be due to aging, neurological disorders, or medication side effects.
Choice D reason: Temperature 37.3°C (99.1°F) is slightly elevated but not indicative of a bladder infection. Older adults may have lower baseline temperatures and may not develop fever in response to an infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Blurred vision is not an expected side effect of digoxin, but a sign of digoxin toxicity, which requires immediate medical attention.
Choice B reason: This is the correct answer because digoxin can cause hypokalemia (low potassium levels), which increases the risk of digoxin toxicity. Therefore, clients taking digoxin need to have their potassium levels monitored regularly and consume foods rich in potassium.
Choice C reason: Antacids can interfere with the absorption of digoxin and reduce its effectiveness. Clients taking digoxin should avoid taking antacids within two hours of taking the medication.
Choice D reason: Weighing oneself every other day is not related to digoxin therapy, but to fluid balance. Clients with heart failure, who are often prescribed digoxin, need to monitor their weight daily and report any significant changes to their health care provider.
Correct Answer is B
Explanation
Choice A reason: Performing breast exams every other month is not an adequate frequency, as it can delay the detection of any changes or abnormalities. The client should perform breast exams monthly, preferably a few days after their period ends.
Choice B reason: Having one breast larger than the other is a common variation and not a cause for concern, unless there is a sudden change in size or shape. The client should be aware of their normal breast appearance and report any changes to their provider.
Choice C reason: Performing breast exams the day their period begins is not an optimal time, as their breasts may be swollen, tender, or lumpy due to hormonal fluctuations. The client should perform breast exams when their breasts are not affected by their menstrual cycle, such as a week after their period ends.
Choice D reason: Having skin dimpling on their breasts is not a common variation and may indicate an underlying tumor that pulls on the connective tissue and causes puckering of the skin. The client should inspect their breasts for any changes in skin texture, such as dimpling, peau d'orange, or redness, and report them to their provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today