A nurse is collecting data from an 18-month-old toddler at a well-child visit.
Which of the following findings should the nurse report to the provider?
The toddler can remove her own socks.
The toddler has a security blanket.
The toddler can say four words.
The toddler throws a ball without falling.
The Correct Answer is C
c. The toddler can say four words.
Explanation:
The nurse should report to the provider that the toddler can say four words. At 18 months, a toddler typically has a vocabulary of about 6 to 20 words and is beginning to combine words into simple phrases. If the toddler is only able to say four words or has a delay in language development, it could be a cause for concern and warrant further evaluation.
The other options are age-appropriate developmental milestones for an 18-month-old toddler and do not require immediate reporting to the provider. The ability to remove socks, having a security blanket, and throwing a ball without falling are all examples of normal developmental skills for a toddler of this age.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Answer: A. Frequently remind the client of the expectations for her behavior.
Rationale:
A) Frequently remind the client of the expectations for her behavior:
Clients experiencing mania may have difficulty maintaining appropriate behavior due to their heightened energy levels and impulsivity. Frequently reminding them of behavioral expectations helps provide structure and boundaries, which can promote a safer and more controlled environment.
B) Encourage the client to participate in a group activity in the dayroom:
While social interaction can be beneficial, clients in a manic state might be overly stimulated by group activities. This can exacerbate their symptoms, leading to increased agitation or disruptive behavior. It's often more appropriate to provide a calm and low-stimulation environment.
C) Allow the client to pick her own choice of clothing:
Allowing a manic client to choose their own clothing can lead to choices that are inappropriate for the setting or the weather, as judgment may be impaired during mania. Providing guidance in clothing choices can help ensure the client is dressed suitably and safely.
D) Encourage the client to increase physical activity during the day:
While physical activity is generally beneficial, clients in a manic state may already be overly active and may not need encouragement to increase their activity. Overexertion can lead to exhaustion and further exacerbate manic symptoms. It is often more beneficial to encourage activities that promote relaxation and calmness.
Correct Answer is B
Explanation
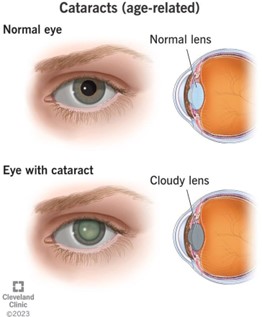
Cloudy vision is a symptom of cataracts. Cataracts occur when the lens of the eye becomes cloudy, causing visual disturbances such as cloudy or blurry vision.The other options are not typical symptoms of cataracts.
a) Sudden dimmed vision may be a symptom of other eye conditions.
c) Intermitent flashes of light (option c) may be a symptom of other eye conditions such as retinal detachment.
d) Pain in the eyes (option d) is not a typical symptom of cataracts.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today