A nurse is collecting data from a newborn who was born 24 hr ago. Which of the following images should the nurse identify as an indication that the newborn has erythema toxicum?
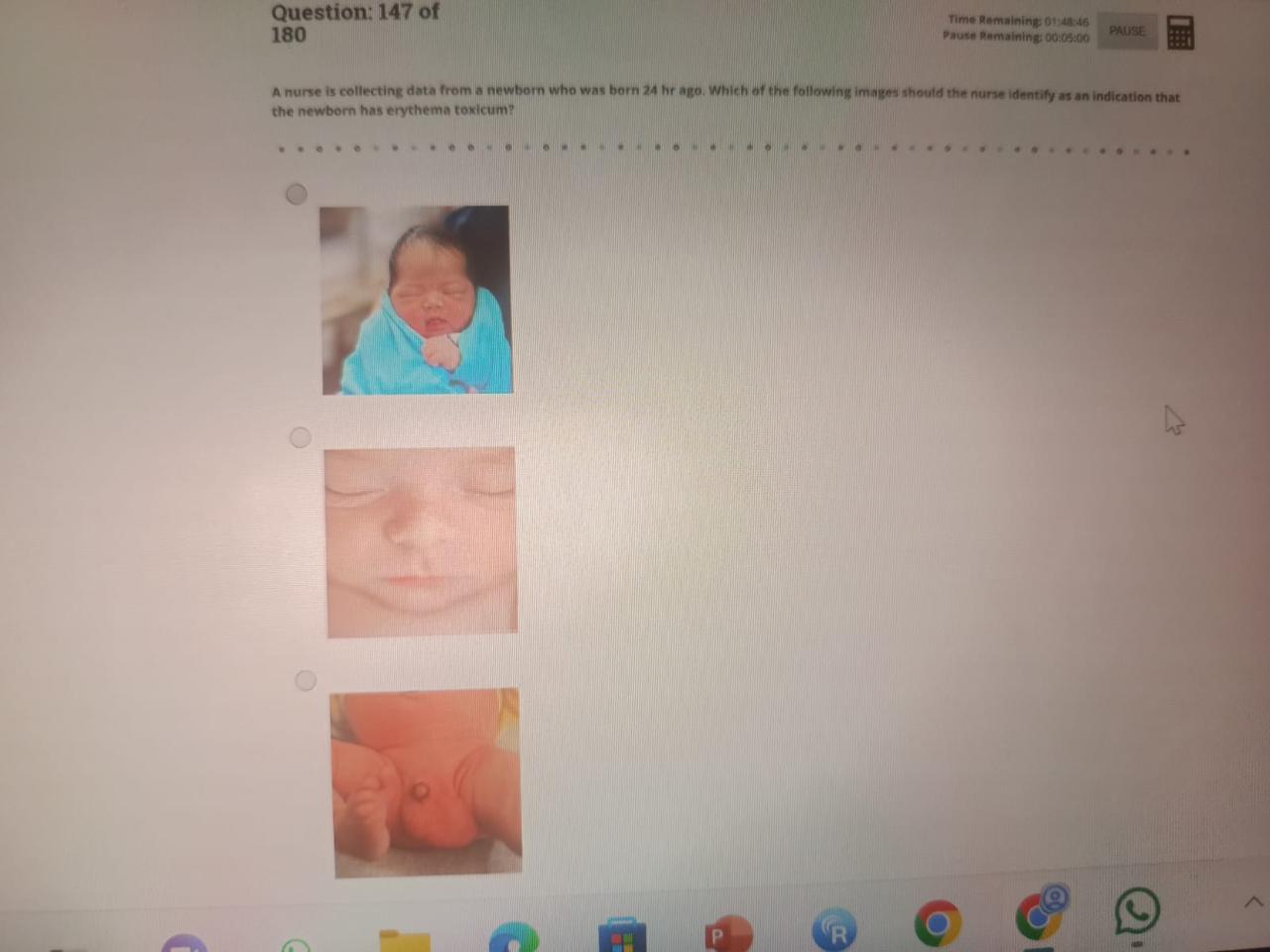
A
B
C
The Correct Answer is B
Rationale:
A. This image shows a newborn with normal skin tone and no visible skin lesions. There are no signs of erythema, pustules, or macules that would suggest erythema toxicum.
B. This image displays multiple small, erythematous macules and papules, especially on the face. These are classic signs of erythema toxicum neonatorum, a common and harmless rash seen in the first days of life.
C. The newborn in this image has generally red skin, which could be due to normal newborn circulation changes or mild erythema, but it lacks the distinctive papular or pustular rash pattern seen in erythema toxicum.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Rationale:
A. This image shows a newborn with normal skin tone and no visible skin lesions. There are no signs of erythema, pustules, or macules that would suggest erythema toxicum.
B. This image displays multiple small, erythematous macules and papules, especially on the face. These are classic signs of erythema toxicum neonatorum, a common and harmless rash seen in the first days of life.
C. The newborn in this image has generally red skin, which could be due to normal newborn circulation changes or mild erythema, but it lacks the distinctive papular or pustular rash pattern seen in erythema toxicum.
Correct Answer is C
Explanation
Rationale:
A. A client who has narcissistic personality disorder and refuses to be alone in their room: Clients with narcissistic personality disorder typically display a need for admiration and may fear abandonment, but they are not at increased risk for physical injury.
B. A client who has social anxiety disorder and refuses to attend group therapy: Avoidance of social settings is a hallmark of social anxiety disorder. While it may lead to isolation, it does not place the client at increased risk for physical injury.
C. A client who has bipolar disorder and exhibits impulsive behaviour: Impulsivity during manic episodes in bipolar disorder can lead to high-risk activities such as reckless driving, substance use, or unsafe sexual behavior. These behaviors significantly elevate the client’s risk for accidental or intentional physical injury.
D. A client who has panic disorder and exhibits paresthesia: Paresthesia, such as tingling or numbness, is a common symptom during panic attacks but does not directly increase the risk for physical injury. While distressing, it typically resolves and is not associated with unsafe behaviors.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today