A nurse is collecting data from a client who is at 29 weeks of gestation.
Which of the following findings should the nurse identify as a potential indication of a prenatal complication?
Leg cramps.
Ptyalism.
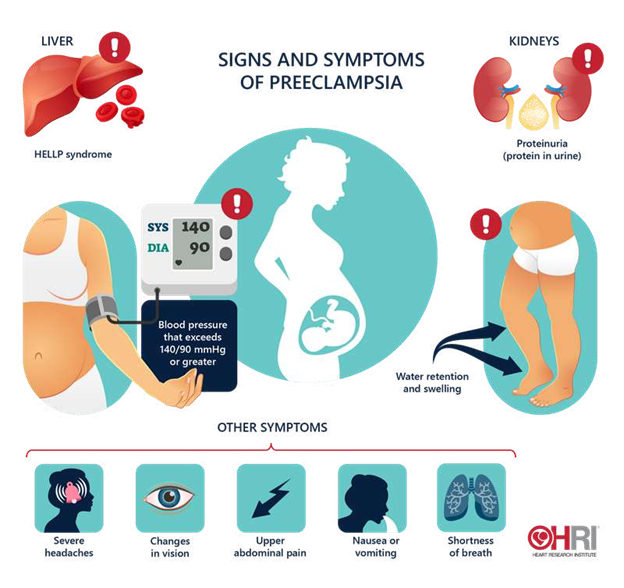
Blurred vision.
Melasma.
The Correct Answer is C
This can be a sign of preeclampsia, a serious complication of pregnancy that causes high blood pressure and proteinuria.
The nurse should report this finding to the provider and monitor the client’s blood pressure, urine protein, and reflexes.
Choice A is wrong because leg cramps are a common discomfort during pregnancy and are not usually a sign of a complication.
Choice B is wrong because ptyalism, or excessive salivation, is a normal physiological change during pregnancy and does not indicate a problem.
Choice D is wrong because melasma, or darkening of the skin on the face, is also a normal physiological change during pregnancy and does not pose a risk to the mother or the fetus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Frequent swallowing after a tonsillectomy may indicate postoperative bleeding. The nurse should check the back of the throat with a pen light to assess for signs of hemorrhage.
B. While obtaining vital signs is important, it does not directly address the concern of potential bleeding.
C. Administering analgesia is appropriate for pain management but does not address the priority concern of bleeding.
D. Offering water could potentially worsen bleeding if it is occurring and should not be the first action.
Correct Answer is B
Explanation
Verapamil is a calcium channel blocker that can lower blood pressure and cause dizziness or fainting, especially when standing up from a sitting or lying position. Changing positions slowly can help prevent these symptoms.
Choice A is wrong because palpitations are not an expected side effect of verapamil, but rather a sign of a possible overdose or a serious heart problem that requires medical attention.
Choice C is wrong because verapamil should be taken with food or milk to avoid stomach upset and increase absorption.
Choice D is wrong because verapamil does not cause weight loss, but rather weight gain as a possible side effect.
Increasing calorie intake is not necessary and may worsen other health conditions such as diabetes or high cholesterol.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today