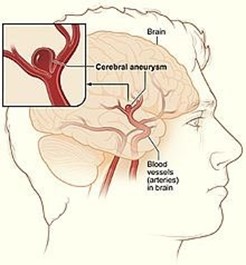
A nurse is collecting data from a client who is 6 days post craniotomy for removal of an intracerebral aneurysm. The nurse should monitor the client for which of the following manifestations of increased intracranial pressure?
Peripheral edema
Diarrhea
Decreased pedal pulses
Hypertension
The Correct Answer is D
A nurse collecting data from a client who is 6 days post craniotomy for removal of an intracerebral aneurysm should monitor the client for hypertension as a manifestation of increased intracranial pressure. Increased intracranial pressure can cause changes in blood pressure, including hypertension.
a. Peripheral edema is not a manifestation of increased intracranial pressure. Peripheral edema is swelling in the extremities and can be caused by a variety of conditions.
b. Diarrhea is not a manifestation of increased intracranial pressure. Diarrhea is loose or watery stools and
can be caused by a variety of conditions.
c. Decreased pedal pulses are not a manifestation of increased intracranial pressure. Decreased pedal
pulses can indicate poor circulation to the feet and can be caused by a variety of conditions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
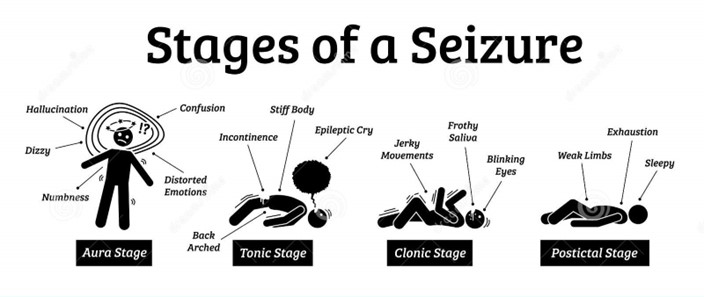
The nurse should use the term "postictal phase" when documenting the client's difficulty arousing and sleepiness for several hours following a generalized tonic-clonic seizure. The postictal phase is the period of time immediately following a seizure during which the client may be difficult to arouse and very sleepy.
Presence of absence seizures, presence of automatisms, and aura phase are not appropriate descriptions for the nurse to use when documenting this finding in the medical record. Absence seizures are a type of seizure characterized by brief episodes of staring and unresponsiveness. Automatisms are repetitive, unconscious movements that can occur during a seizure. The aura phase is a warning sign that can occur before a seizure.
Correct Answer is C
Explanation
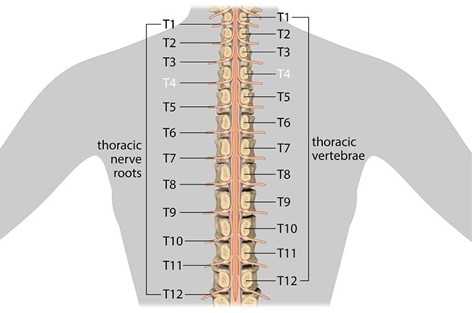
To prevent autonomic dysreflexia, the nurse should take the intervention of preventing bladder distention. Autonomic dysreflexia is a serious medical problem that can happen if a person has injured the spinal cord in their upper back¹. It makes their blood pressure dangerously high and can lead to a stroke, seizure, or cardiac arrest¹. One way to lower the chance of complications is to use the bathroom on a regular schedule and keep the bladder and bowels from becoming too full.
a. Monitoring for elevated blood pressure is important but not an intervention to prevent autonomic dysreflexia.
b. Providing analgesia for headaches is important but not an intervention to prevent autonomic dysreflexia.
d. Elevating the client's head is important but not an intervention to prevent autonomic dysreflexia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today