A nurse is caring for an infant who has gastroenteritis.
Which of the following assessment findings should the nurse report to the provider?
Sunken fontanels and dry mucous membranes.
Temperature 38° C (100.4° F) and pulse rate 124/min.
Decreased appetite and irritability.
Pale and a 24-hr fluid deficit of 30 mL.
The Correct Answer is A
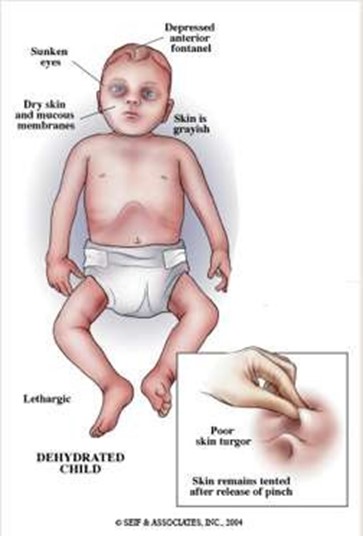
These are signs of severe dehydration in an infant, which can be life-threatening and should be reported to the provider immediately. The infant may need intravenous fluids and electrolytes to restore hydration and prevent complications.
Choice B is wrong because a temperature of 38° C (100.4° F) and a pulse rate of 124/min are not abnormal for an infant and do not indicate severe dehydration. These are common findings in an infant who has gastroenteritis, which is an inflammation of the stomach and intestines caused by a virus, bacteria, or parasite.
Choice C is wrong because decreased appetite and irritability are also common findings in an infant who has gastroenteritis, but they do not indicate severe dehydration. The nurse should encourage oral rehydration with fluids such as breast milk, formula, or oral electrolyte solution.
Choice D is wrong because pale skin and a 24-hr fluid deficit of 30 mL are not signs of severe dehydration in an infant.
A fluid deficit of 30 mL is less than 1 oz and is not significant for an infant who weighs about 10 kg (22 lbs). A fluid deficit of more than 10% of body weight would indicate severe dehydration.
Normal ranges for vital signs in infants are as follows:
• Temperature: 36.5° C to 37.5° C (97.7° F to 99.5° F)
• Pulse rate: 100 to 160/min
• Respiratory rate: 30 to 60/min
• Blood pressure: 65/41 to 100/50 mm Hg
Normal ranges for fluid intake and output in infants are as follows:
• Fluid intake: 100 to 150 mL/kg/day
• Fluid output: 1 to 2 mL/kg/hr
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation

This is because glass ampules can leave small shards of glass in the solution, which can be harmful if injected into the client. A filter needle has a small mesh that traps any glass particles and prevents them from entering the syringe.
Choice B is wrong because the nurse should break the neck of the ampule away from the body to avoid injury from the glass.
Choice C is wrong because the nurse should use a different needle to inject the client after withdrawing the medication with a filter needle. This is to prevent contamination and reduce pain for the client.
Choice D is wrong because the nurse should dispose of the ampule in a sharps container, not in the trash can. This is to prevent injury and infection from the broken glass.
Correct Answer is {"A":{"answers":"A"},"B":{"answers":"B"},"C":{"answers":"B"},"D":{"answers":"B"},"E":{"answers":"B"}}
Explanation
The correct answer is choice A. Applying warm compresses to the incision site is anticipated for the client, as it can help reduce swelling and pain.
The other choices are contraindicated for the following reasons:
- Choice B: Maintaining bed rest for 2 days postoperatively is contraindicated, as it can increase the risk of complications such as deep vein thrombosis, pulmonary embolism, and pneumonia. The client should be encouraged to ambulate as soon as possible after surgery.
- Choice C: Irrigating indwelling urinary catheter with 50 mL of normal saline is contraindicated, as it can introduce bacteria into the bladder and cause infection. The catheter should be kept patent and draining without irrigation unless there is a specific order from the provider.
- Choice D: Administering enema to relieve constipation is contraindicated, as it can increase the pressure in the pelvic area and cause bleeding or damage to the surgical site. The client should be given stool softeners and laxatives to prevent constipation.
- Choice E: Placing a blanket roll under the client’s knees while in bed is contraindicated, as it can impair blood circulation and cause thrombophlebitis. The client should avoid flexing the knees excessively and elevate the legs slightly when lying down.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today