A nurse is caring for a client who is scheduled for surgery. While the nurse is witnessing the client's signature, the client states, "I trust my doctor, but I don't understand what is meant by resecting my intestines." Which of the following actions should the nurse take?
Notify the provider.
Describe the surgery to the client.
Provide brochures about the procedure.
Complete an incident report.
The Correct Answer is A
Choice A reason:
The client has expressed a lack of understanding about the procedure, which indicates that they may not have received sufficient information or clarification. It is important to notify the provider so they can ensure the client fully understands the procedure before giving informed consent.
Choice B reason:
The nurse should provide basic information and answer questions within their scope, but detailed explanations about the procedure are best provided by the provider who is performing the surgery.
Choice C reason:
While brochures can be helpful, they do not replace the need for direct, clear communication with the healthcare provider about the specific details of the surgery.
Choice D reason:
An incident report is not necessary in this context as the situation is related to informed consent and not an error or safety issue.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason:
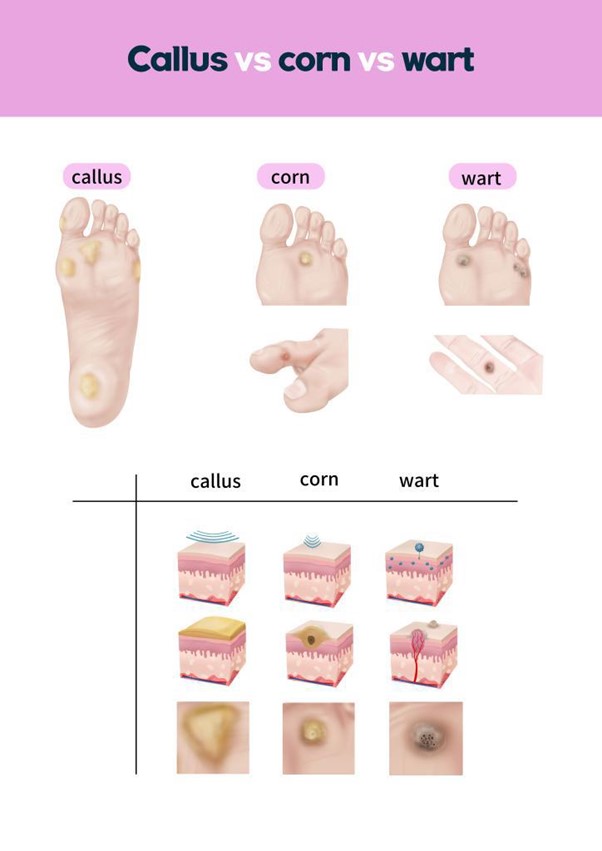
Soaking feet in warm water daily is not recommended for individuals with diabetes, as it can increase the risk of skin maceration and infection. People with diabetes should be cautious about foot care practices that involve prolonged moisture exposure.
Choice B reason:
Placing an oval corn pad over the toes with corn and removing it weekly may not be the best approach, as it can increase pressure on the area and potentially cause further skin irritation.
Choice C reason:
Using over-the-counter liquid medication to remove corns is not recommended for individuals with diabetes, as it can cause skin irritation, burns, or infection. It's important for individuals with diabetes to seek professional guidance for proper foot care.
Choice D reason:
"I can apply lotion to soften calluses as long as I don't put lotion between my toes." This is the correct statement. This statement indicates an understanding of proper care for corns and calluses. Applying lotion to soften calluses can help reduce discomfort, but it's important to avoid putting lotion between the toes to prevent excess moisture build-up that could lead to skin breakdown or infection.
Correct Answer is D
Explanation
A. Develop a plan for the client to integrate the change into her lifestyle: Developing a plan for integrating change into one's lifestyle is more appropriate during the preparation stage when the client is actively planning to make a change. During the contemplation stage, the focus is on considering change rather than developing a detailed plan.
B. Assist the client in setting goals to make the change: Setting specific goals is more appropriate during the preparation stage when the client is actively planning to make a change. During the contemplation stage, the client is not yet ready to commit to specific goals.
C. Recommend small changes for the client to make to change her behavior over time: During the contemplation stage of health behavior change, clients are considering making a change but are not yet committed to taking immediate action. This is also more suitable for the preparation or action stages.
D. In the contemplation stage, the client is aware of the problem and is considering making a change but has not yet committed to action. Providing information about the benefits can help the client move toward the next stage of change.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today