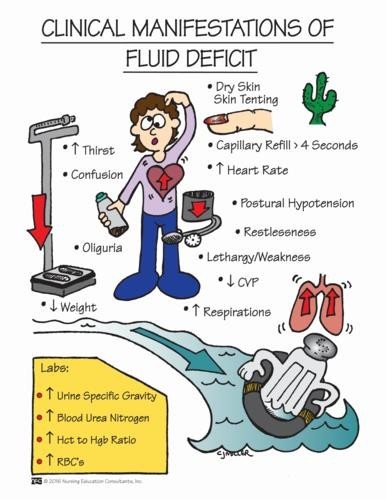
A nurse is caring for a client who is postoperative and is experiencing nausea and vomiting. The nurse should identify which of the following findings as indications that the client has fluid volume deficit. (Select all that apply.)
Full bounding pulse
Cool extremities
Moist crackles in the lungs
Orthostatic hypotension
Flat neck veins
Correct Answer : B,D,E
A: A full bounding pulse is a sign of increased fluid volume or fluid overload, not fluid volume deficit.
B: Cool extremities can be an indication of decreased peripheral perfusion, which may occur in fluid volume deficit.
C: Moist crackles in the lungs are an indication of fluid volume excess or pulmonary congestion, not fluid volume deficit.
D: Orthostatic hypotension, which is a drop in blood pressure when changing from lying to standing, can be a sign of fluid volume deficit due to inadequate blood volume.
E: Flat neck veins are an indication of decreased venous return and can occur in fluid volume deficit.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is {"dropdown-group-1":"C","dropdown-group-2":"E"}
Explanation
The nurse should first review the medications that may be causing the client's confusion, as certain drugs can contribute to altered mental status and should be promptly identified and addressed. After identifying and managing the cause, the nurse should focus on using alternative methods to keep the client safe, ensuring both immediate and long-term patient safety, especially if medication adjustments are required.
Correct Answer is B
Explanation
A. Empty the urine drainage bag every 12 hours: While it's essential to empty the urine drainage bag regularly to prevent it from becoming too full, emptying it every 12 hours alone is not sufficient to prevent urinary tract infections (UTIs).
B. Drain the urine from the tubing before ambulation: Correct. Before the client ambulates or moves, the nurse should ensure that the urinary catheter's tubing is emptied. This prevents urine from flowing back into the bladder, reducing the risk of UTIs.
C. Use clean technique for urine specimen collection: While using clean technique during urine specimen collection is important for preventing contamination, it is not the primary action needed to prevent UTIs in a client with an indwelling urinary catheter.
D. Hang the urine drainage bag at the level of the bladder: While proper positioning of the drainage bag is essential for optimal urine flow and to prevent backflow, it alone is not sufficient to prevent UTIs.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today