A nurse is caring for a client who is in labor. The nurse observes late decelerations of the fetal heart rate on the external fetal monitor. After placing the client in a side-lying position, which of the following actions should the nurse take?
Perform fetal scalp stimulation
Administer oxygen via a face mask.
Elevate the client's head.
Decrease the rate of IV fluids.
The Correct Answer is B
A. Perform fetal scalp stimulation:
Fetal scalp stimulation involves applying pressure to the fetal scalp during a vaginal examination to elicit a response from the fetus, such as an acceleration of the fetal heart rate. While this can provide additional information about fetal well-being, it is not the initial priority when late decelerations are observed on the fetal monitor. The focus should first be on interventions aimed at improving fetal oxygenation to address the underlying cause of the late decelerations.
B. Administer oxygen via a face mask:
Administering oxygen to the mother is a priority intervention when late decelerations of the fetal heart rate are observed on the external fetal monitor. Late decelerations often indicate uteroplacental insufficiency, where the fetus is not receiving adequate oxygenation. Administering oxygen to the mother helps increase oxygen levels in her blood, improving oxygen delivery to the fetus and potentially mitigating the effects of uteroplacental insufficiency.
C. Elevate the client's head:
Elevating the client's head is not indicated when late decelerations are observed. This position could potentially compromise maternal-fetal circulation by reducing blood flow to the placenta. Maintaining a side-lying or semi-Fowler's position is often recommended to improve blood flow to the placenta and enhance fetal oxygenation.
D. Decrease the rate of IV fluids:
Adjusting the rate of IV fluids may be considered in some situations, such as if there is evidence of fluid overload or if the mother is receiving excessive amounts of IV fluids. However, it is not typically the initial intervention for addressing late decelerations. The focus should first be on interventions aimed at improving maternal-fetal oxygenation, such as administering oxygen and positioning the client appropriately.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Human papillomavirus (HPV) vaccine:
The HPV vaccine is not recommended during pregnancy because there is limited safety data regarding its use in pregnant women. It is typically administered to individuals before they become sexually active to prevent HPV infections, which can lead to cervical cancer and other HPV-related diseases. Since the client is currently pregnant, administering the HPV vaccine would not be appropriate due to the lack of safety data during pregnancy.
B. Rubella vaccine:
The rubella vaccine is a live attenuated vaccine, and its administration during pregnancy is contraindicated due to the risk of congenital rubella syndrome (CRS) if the vaccine were to cause rubella infection in the pregnant woman. Rubella vaccination should be provided to non-pregnant individuals, particularly women of childbearing age, to prevent CRS. Administering the rubella vaccine to a pregnant woman at 28 weeks of gestation would pose a risk to both the mother and the developing fetus.
C. Varicella vaccine:
Similar to the rubella vaccine, the varicella (chickenpox) vaccine is a live attenuated vaccine and is contraindicated during pregnancy due to the risk of varicella infection in the pregnant woman, which can lead to severe complications for both the mother and the fetus. Varicella vaccination is recommended for individuals who have not had chickenpox or received the vaccine previously but should not be administered to pregnant women.
D. Tetanus vaccine:
Tetanus vaccination during pregnancy is recommended to prevent maternal and neonatal tetanus. Tetanus toxoid is considered safe during pregnancy and is routinely administered as part of the tetanus-diphtheria-pertussis (Tdap) vaccine. The tetanus vaccine helps protect against tetanus, a potentially fatal bacterial infection. Administering the tetanus vaccine during pregnancy is important for the health and safety of both the mother and the developing fetus.
Correct Answer is B
Explanation
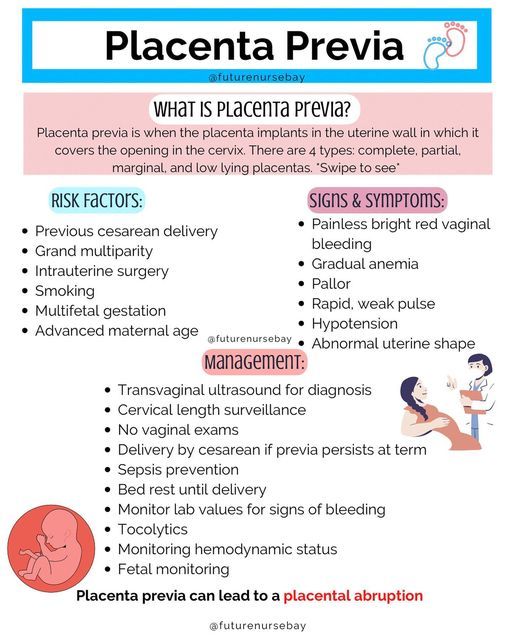
A. Uterine hypertonicity:
Uterine hypertonicity, or excessive uterine contractions, is not typically associated with placenta previa. In fact, placenta previa can be complicated by uterine relaxation due to the placental attachment over the cervix, which can lead to painless vaginal bleeding.
B. Painless, vaginal bleeding:
Painless vaginal bleeding, particularly in the third trimester, is a hallmark sign of placenta previa. This bleeding occurs due to the disruption of blood vessels in the placenta as the cervix begins to dilate or efface, causing blood to flow past the placenta and out of the vagina without associated uterine contractions or abdominal pain.
C. Firm, rigid abdomen:
A firm, rigid abdomen is not a typical finding in placenta previa. Instead, the abdomen is usually soft and nontender unless there are complications such as uterine rupture or hemorrhage, which are rare but serious complications of placenta previa.
D. Persistent headache:
While persistent headache can be a symptom of certain pregnancy complications such as preeclampsia, it is not a specific finding associated with placenta previa. Headache alone is not typically associated with placenta previa unless it is accompanied by other signs of preeclampsia or complications related to severe hemorrhage.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today