A nurse is caring for a client who has a placenta previa. Which of the following findings should the nurse expect?
Nausea.
Polyhydramnios.
Uterine tenderness.
Spotting.
The Correct Answer is D
Placenta previa is a condition where the placenta implants in the lower part of the uterus, partly or completely covering the cervical opening.
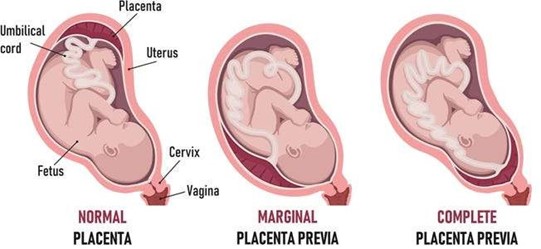
This can cause painless, bright red vaginal bleeding, usually in the third trimester. Spotting is a sign of placenta previa and should be reported to the provider immediately. Choice A is wrong because nausea is not a specific finding of placenta previa.
Nausea can occur in normal pregnancy or in other conditions such as hyperemesis gravidarum or preeclampsia.
Choice B is wrong because polyhydramnios is not a finding of placenta previa.
Polyhydramnios is a condition where there is too much amniotic fluid in the uterus, which can cause complications such as preterm labor, cord prolapse, or fetal malformations.
Choice C is wrong because uterine tenderness is not a finding of placenta previa.
Uterine tenderness is a sign of abruptio placentae, which is a condition where the placenta separates from the uterine wall before delivery.
This can cause severe abdominal pain, dark red vaginal bleeding, and fetal distress.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["C","E"]
Explanation
Preterm pre-labor rupture of membranes (PROM) is the spontaneous rupture of the amniotic sac before the onset of labor in a pregnancy less than 37 weeks gestation. It can lead to
infection, cord prolapse, placental abruption, and preterm delivery. The client has risk factors for PROM such as a history of preterm birth and a current infection indicated by fever.
Sepsis is a life-threatening condition that occurs when the body’s response to an infection causes damage to its own tissues and organs. The client has signs of sepsis such as fever, tachycardia, and possible organ dysfunction. The client may have a urinary tract infection, a common cause of sepsis in pregnancy, or an intrauterine infection due to PROM or other factors.
Preeclampsia is not a likely complication for this client because she does not have high blood pressure or proteinuria, which are the defining features of preeclampsia. Seizures are not a likely complication for this client because she does not have epilepsy or eclampsia, which are the leading causes of seizures in pregnancy. Placenta previa is not a likely complication for this client because she does not have painless vaginal bleeding, which is the hallmark symptom of placenta previa.
Correct Answer is B
Explanation
Choice A rationale: Adjusting medication times based solely on convenience violates the prescribed dosing interval, which is essential for maintaining therapeutic drug levels and preventing antibiotic resistance or toxicity.
Choice B rationale: Facility policies typically allow a "grace period" for non-time-critical medications, usually 30 to 60 minutes before or after the scheduled time, to ensure safe and timely administration.
Choice C rationale: Administering a medication 2 hours late significantly deviates from the prescribed schedule, potentially causing the drug's plasma concentration to fall below the minimum effective level required for treatment.
Choice D rationale: Increasing the infusion rate of vancomycin is dangerous and can cause "Red Man Syndrome," a hypersensitivity reaction characterized by flushing, rash, and hypotension due to rapid histamine release.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today