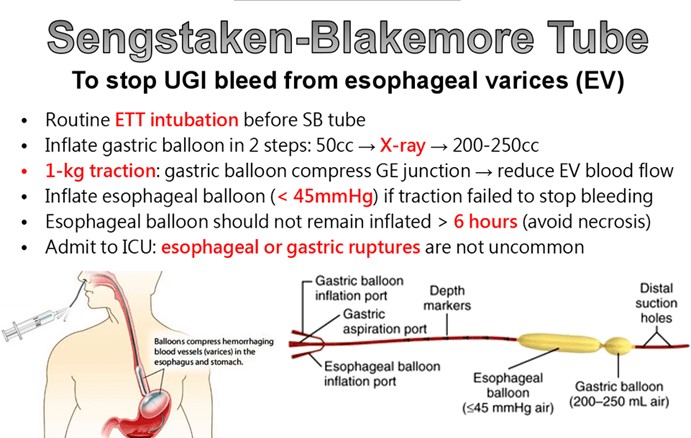
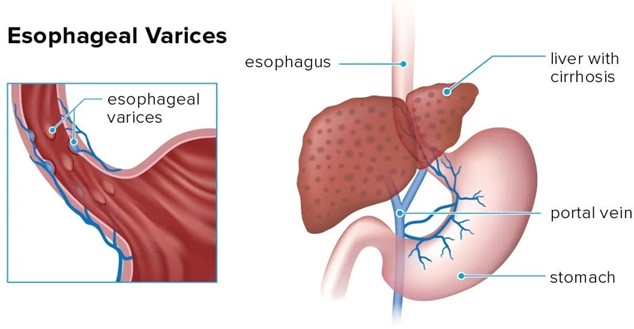
A nurse is caring for a client who has bleeding esophageal varices and is being treated with a Sengstaken-Blakemore tube. Which of the following actions should the nurse perform?
Deflate the balloons for 5 min every 2 hr to prevent tissue necrosis.
Keep the head of the bed flat at all times to prevent the development of shock.
Maintain constant observation while the balloons are inflated.
Suction the tube every 2 hr and as needed to maintain patency.
The Correct Answer is C
Choice A Reason: This is incorrect. The balloons should not be deflated without a physician's order, as this can cause rebleeding or aspiration.
Choice B Reason: This is incorrect. The head of the bed should be elevated to 30 to 45 degrees to reduce pressure on the balloons and prevent gastric reflux.
Choice C Reason: This is correct. The nurse should monitor the client closely for signs of complications, such as airway obstruction, aspiration, or balloon rupture. The nurse should also keep scissors at the bedside to cut the tube and release the balloons in case of an emergency.
Choice D Reason: This is incorrect. The tube should not be suctioned, as this can damage the mucosa and cause bleeding. The nurse should only aspirate gastric contents through the gastric lumen to decompress the stomach.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because this client has signs of brain death, such as severe head injuries, low respiratory rate, and unresponsiveness. The nurse should tag this client as black, which means deceased or expectant.
Choice B Reason: This is incorrect because this client has non-life-threatening injuries, such as a simple fracture and scratches. The nurse should tag this client as green, which means minor or delayed care.
Choice C Reason: This is incorrect because this client has minor injuries and is able to walk around. The nurse should tag this client as green, which means minor or delayed care.
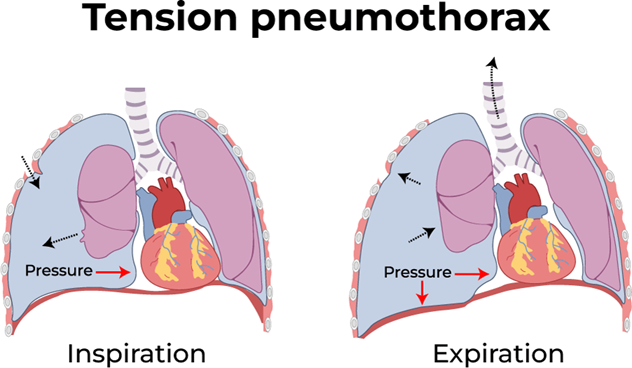
Choice D Reason: This is correct because this client has a life-threatening condition called tension pneumothorax, which requires immediate care. This client has a life-threatening condition called tension pneumothorax, which is caused by air leaking into the pleural space and compressing the lung and the heart. This can lead to respiratory failure, cardiac arrest, and death if not treated immediately. The hissing sound indicates that air is escaping from the lung through the wound. The nurse should tag this client as red, which means immediate care is needed.
Correct Answer is A
Explanation
Choice A: Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
Choice B: Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high-Fowler's position.
Choice C: Ambulating the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
Choice D: Encouraging the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain a nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today