A nurse is caring for a client who has a traumatic brain injury. The client, who has been quiet and cooperative, becomes agitated and restless.
Which of the following assessments should the nurse perform first?
Motor responses.
Blood glucose.
Urinary output.
Blood pressure.
The Correct Answer is D

A change in behavior such as agitation and restlessness in a client with a traumatic brain injury can be a sign of increased intracranial pressure.
The nurse should first assess the client’s blood pressure as an increase in blood pressure can be an indicator of increased intracranial pressure.
Motor responses are not the first assessment that should be performed.
Blood glucose is not the first assessment that should be performed.
Urinary output is not the first assessment that should be performed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This statement indicates an understanding of the teaching because shaking the inhaler helps to mix the medicine inside the canister.
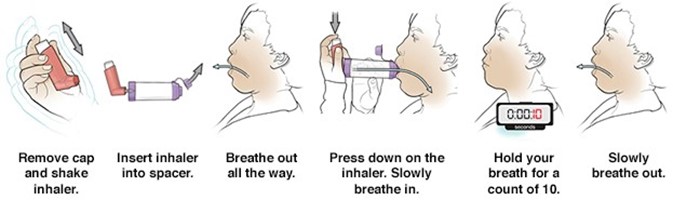
Choice A is incorrect because it is not necessary to clean the cap of the inhaler once per week.
Instead, it is important to clean the inhaler at least once a week or as directed.
Choice B is incorrect because one should inhale the medication slowly, not quickly.
Choice D is incorrect because one should wait 1 minute between puffs, not 15 seconds.
Correct Answer is D
Explanation
Initiate a referral for the client to a home health agency.
This action demonstrates client advocacy because it empowers the client to continue self-care at home while also providing them with additional support and resources through the home health agency.
Choice A is wrong because avoiding large crowds of people is a precautionary measure but does not demonstrate client advocacy.
Choice B is wrong because avoiding raw vegetables is a dietary recommendation but does not demonstrate client advocacy.
Choice C is wrong because reminding the client of the importance of medication adherence is important but does not demonstrate client advocacy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today