A nurse is caring for a client who has a spinal cord injury and has developed autonomic dysreflexia. Identify the sequence of steps the nurse should take.
(Move the steps into the box on the right, placing them in the order of performance. Use all the steps.)
Administer an antihypertensive medication intravenously.
Confirm that the client's bladder is empty.
Indicate the risk for autonomic dysreflexia in the client's medical record.
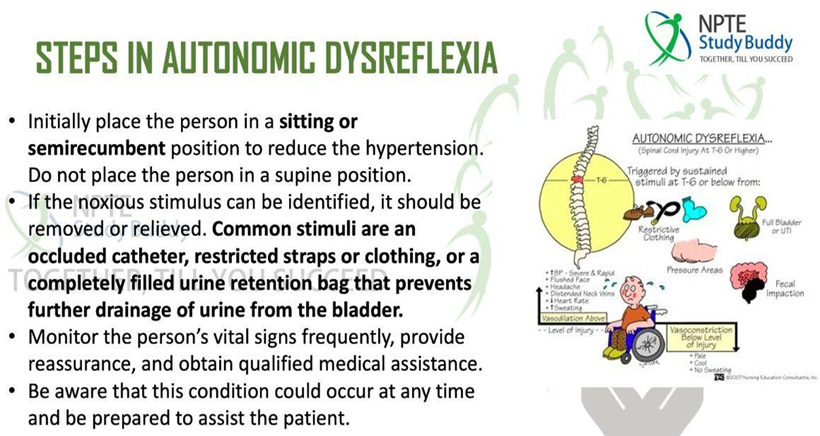
Place the client in an upright sitting position.
The Correct Answer is D,B,A,C
Step D (Place the client in an upright sitting position): Elevating the client's head and upper body to an upright position helps to reduce blood pressure by promoting venous pooling in the lower extremities.
Step B (Confirm that the client's bladder is empty): Autonomic dysreflexia is often triggered by bladder distention or urinary retention. By confirming and addressing urinary issues promptly, the nurse can remove the triggering stimulus.
Step A (Administer an antihypertensive medication intravenously): In severe cases where blood pressure remains dangerously high despite other interventions, such as positioning and addressing bladder issues, antihypertensive medications may be necessary to lower blood pressure quickly and prevent complications.
Step C (Indicate the risk for autonomic dysreflexia in the client's medical record): Documentation of the occurrence of autonomic dysreflexia, its triggers, and interventions used is essential for continuity of care. It informs other healthcare providers about the client's condition and helps in implementing preventive strategies.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A Pain typically occurs when the stomach is empty (1-3 hours after eating), often during the night and early morning. This pattern occurs because the presence of food helps to buffer gastric acid, whereas an empty stomach allows acid to directly contact the ulcerated area, leading to pain.
B. Pain in the right lower quadrant is not typically associated with peptic ulcer disease. Pain in PUD is usually located in the epigastric region (upper abdomen), although it can radiate to the back or other areas depending on the location and severity of the ulcer.
C. Constipation is not a typical finding in peptic ulcer disease. PUD is primarily associated with gastrointestinal symptoms related to acid-peptic imbalance, such as abdominal pain, bloating, nausea, and sometimes vomiting. Bowel habits are generally not directly affected by PUD.
D. In peptic ulcer disease, pain is usually relieved by eating or taking antacids. This is because food intake neutralizes gastric acid and provides a temporary protective coating over the ulcer, reducing irritation and pain.
Correct Answer is A
Explanation
A. Nuchal rigidity refers to stiffness or resistance to neck movement, especially when the client's head is flexed forward. It is a classic sign of meningitis due to irritation and inflammation of the meninges (the membranes surrounding the brain and spinal cord). This assessment helps to detect meningeal irritation, a hallmark of meningitis.
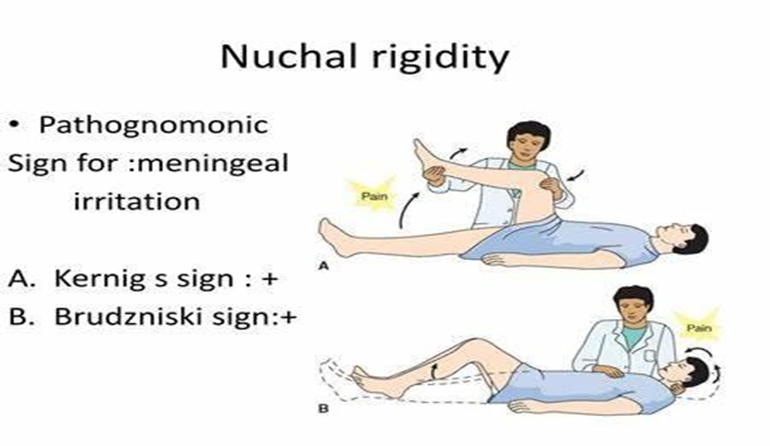
B. This action tests the deep tendon reflex, specifically the knee jerk reflex (patellar reflex). It assesses the integrity of the spinal cord and peripheral nerves. While it is part of a neurological assessment, it is not specifically related to the assessment of meningitis unless there are concurrent neurological symptoms or signs.
C This maneuver tests for Babinski reflex, which is an abnormal response where the toes flare upward and the big toe dorsiflexes when the sole of the foot is stimulated. A positive Babinski reflex can indicate dysfunction of the corticospinal tract or brain injury but is not a specific finding in meningitis.
D. Tapping the facial nerve (cranial nerve VII) assesses for the presence of facial nerve irritation or damage. In the context of meningitis, signs such as facial twitching or asymmetry may indicate involvement of cranial nerves due to inflammation and pressure within the skull.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today