A nurse is assisting with the development of a plan of care for an older adult who is at risk for falls. Which of the following actions should the nurse contribute to the plan? (Select all that apply)
Keep the bed at a comfortable working height.
Administer a sedative at bedtime.
Keep a night light on in the client's room and bathroom.
Place the bedside table within the client's reach.
Lock the wheels on beds and wheelchairs during transfers.
Correct Answer : C,D,E
Keeping a night light on in the client's room and bathroom can help reduce the risk of falls by improving visibility and orientation at night. Placing the bedside table within the client's reach can help reduce the risk of falls by making it easier for the client to access necessary items without having to get up and move around. Locking the wheels on beds and wheelchairs during transfers can help reduce the risk of falls by providing stability and preventing unwanted movement.
a. Keeping the bed at a comfortable working height is important for the nurse's comfort and safety while providing care, but it does not directly reduce the risk of falls for the client.
b. Administering a sedative at bedtime may help the client sleep, but it can also increase the risk of falls by causing drowsiness and disorientation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The nurse should monitor the client for lethargy as a manifestation of increased intracranial pressure. Increased intracranial pressure (ICP) is a rise in pressure around the brain that can occur due to various reasons such as brain injury, bleeding into the brain, swelling in the brain, or an increase in cerebrospinal fluid². Lethargy (feeling less alert than usual) is a common symptom of increased ICP⁴.
Nuchal rigidity is not a common symptom of increased ICP.
Batle's sign is not a common symptom of increased ICP.
Polyuria is not a common symptom of increased ICP.

Correct Answer is B
Explanation
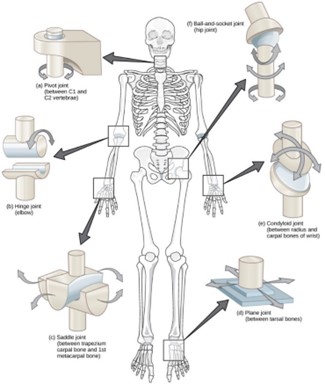
The knee is a hinge type of joint. When describing range-of-motion exercises, the nurse should explain that the knee is a hinge joint. A hinge joint is a type of synovial joint that mainly allows for flexion and extension (and a small degree of medial and lateral rotation)¹. The knee joint is formed by articulations between the patella, femur, and tibia¹.
a. The knee is not a pivot joint.
c. The knee is not a ball and socket joint.
d. The knee is not a gliding joint.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today