A nurse is assisting with the admission of an older adult client who has impaired mobility and is at risk for falls. Which of the following actions should the nurse plan to perform first?
Check the client's ability to use the call light.
Document the client's risk in the medical record.
Request a referral for physical therapy
Place a gait belt in the client's room.
The Correct Answer is A
The first action the nurse should plan to perform is to check the client's ability to use the call light. This is essential to ensure that the client can easily communicate with the healthcare team if they need assistance or experience a fall risk situation. By confirming the client's ability to use the call light, the nurse can address any potential communication barriers and ensure that the client has a means to request help promptly.
Explanation for the other options:
b) Document the client's risk in the medical record: While documenting the client's risk in the medical record is important, it is not the first action to be taken. Ensuring the client's immediate safety and ability to request assistance is the priority.
c) Request a referral for physical therapy: Referring the client for physical therapy may be a necessary step to address their impaired mobility and reduce fall risk, but it is not the first action to be performed. Assessing their ability to use the call light takes precedence in order to address immediate safety concerns.
d) Place a gait belt in the client's room: Providing a gait belt is a measure to assist with mobility and falls prevention. However, it should not be the first action. Checking the client's ability to use the call light is more critical to ensure their immediate safety and ability to request help.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
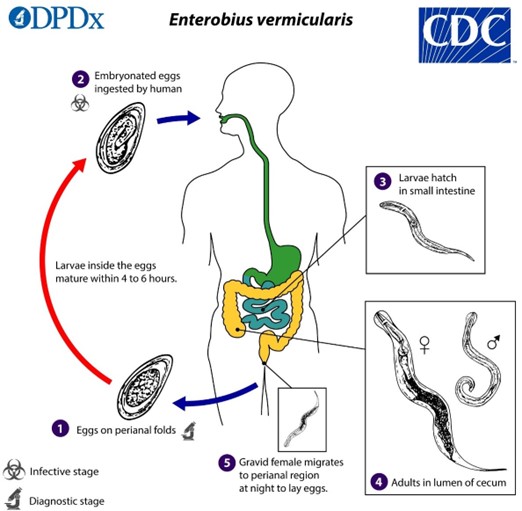
b. "Everyone who lives in the home will need medication."
The nurse should inform the guardian that everyone who lives in the home will need medication when reinforcing teaching about enterobiasis. Enterobiasis, also known as pinworm infection, is highly contagious, and it can easily spread from person to person within the household. Treating only the affected individual may not be sufficient to eliminate the infection completely, as other household members may also be infected or at risk of reinfection.
Explanation for the other options:
a. "One dose of medication is all that will be necessary." Enterobiasis is typically treated with a medication regimen that involves taking multiple doses over a period of time. This is to ensure that all stages of the pinworm life cycle are targeted and eradicated. A single dose is usually not sufficient to eliminate the infection completely.
c. "Allow the child to take tub baths instead of showers." The choice of tub baths or showers does not directly impact the treatment or prevention of enterobiasis. Both methods of bathing can be used, but it is important to maintain good hygiene practices, such as regular handwashing and proper cleaning of the perianal area, to reduce the risk of reinfection.
d. "Wash all clothes and bed linens in cold water." While proper hygiene practices and laundering of clothes and bed linens are important in preventing the spread of enterobiasis, using cold water alone may not be sufficient. Washing clothes and bed linens in hot water (at a temperature of at least 60°C or 140°F) is recommended to kill any pinworm eggs that may be present.
Correct Answer is A
Explanation
The correct answer is a. Call EMS if a seizure lasts 5 minutes or more.
Explanation:
When providing home care instructions for a child with a seizure disorder, it is important to educate the parents about appropriate actions during a seizure. Calling emergency medical services (EMS) if a seizure lasts 5 minutes or more is crucial because it may indicate a condition called status epilepticus, which is a prolonged seizure or a series of seizures without full recovery of consciousness between them. Status epilepticus is a medical emergency that requires immediate medical intervention.
Option b, restraining the child at the onset of a seizure, is not recommended. Restraint can potentially cause harm to the child and increase the risk of injury. It is advised to create a safe environment by removing any nearby objects that could cause injury and placing a pillow or cushion under the child's head to prevent head injury.
Option c, offering the child a bubble bath every evening, is not specifically related to seizure management. Bathing routines can be continued as long as they are safe and supervised. However, it is important to ensure the child's safety during bathing, such as providing adequate supervision to prevent drowning or injury.
Option d, placing the child in a prone position during a seizure, is not recommended. Placing the child in a prone position (face down) during a seizure can obstruct the airway and increase the risk of respiratory complications. The child should be placed on their side, in a recovery position, to facilitate drainage of saliva or other fluids and prevent choking.
Overall, the most important instruction for the parents is to recognize the signs of prolonged seizure activity and to seek immediate medical assistance by calling EMS if a seizure lasts 5 minutes or more.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today