A nurse is assessing a client with eclampsia who is having a seizure.
Which of the following actions should the nurse take first?
Turn the client to the side
Insert an oral airway
Administer oxygen via face mask
Document the duration of the seizure
The Correct Answer is A
Turn the client to the side. This is because turning the client to the side will prevent aspiration and maintain a patent airway during a seizure.
Some possible explanations for the other choices are:
• Choice B. Insert an oral airway. This is wrong because inserting an oral airway during a seizure can cause injury to the client’s mouth or teeth, and it can also stimulate the gag reflex and increase the risk of vomiting and aspiration.
• Choice C. Administer oxygen via face mask. This is wrong because administering oxygen via face mask during a seizure can be difficult and ineffective, as the client may not be able to breathe through the mask or may dislodge it with their movements. Oxygen can be given after the seizure has stopped, if needed.
• Choice D. Document the duration of the seizure.
This is wrong because documenting the duration of the seizure is not a priority action during a seizure. The nurse should first ensure the client’s safety and airway patency, and then document the seizure characteristics after it has ended.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","C","E"]
Explanation
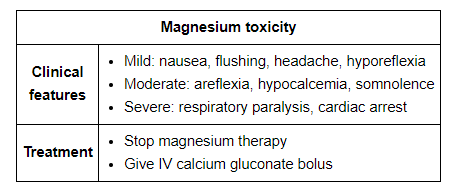
The correct answer is choice A, B, C and E.The nurse should monitor the client’s deep tendon reflexes hourly because magnesium sulfate can cause neuromuscular blockade and decreased reflexes.The nurse should keep calcium gluconate readily available because it is the antidote for magnesium toxicity.The nurse should maintain a urine output of at least 40 mL/hr because magnesium is excreted by the kidneys and low urine output can indicate renal impairment or fluid overload.The nurse should check the client’s blood pressure every 15 minutes because magnesium sulfate can cause hypotension and preeclampsia can cause hypertension.
Choice D is wrong because the medication should not be infused via a peripheral IV line, but rather through a central line or a large-bore IV catheter to prevent tissue damage.
Correct Answer is A
Explanation
This indicates that the client has respiratory depression, which is a sign of magnesium toxicity.Magnesium sulfate is given to prevent and treat seizures in clients with eclampsia, but it can also cause adverse effects such as hypotension, decreased urine output, absent or diminished reflexes, and cardiac arrest.
Choice B is wrong because urine output of 50 mL/hr is within the normal range and does not indicate magnesium toxicity.The nurse should monitor the client’s urine output closely and report any decrease below 30 mL/hr.
Choice C is wrong because serum magnesium level of 6 mg/dL is within the therapeutic range of 4 to 7 mg/dL for clients receiving magnesium sulfate.The nurse should monitor the client’s serum magnesium level regularly and report any increase above 8 mg/dL, which indicates toxicity.
Choice D is wrong because patellar reflex of 2+ is normal and does not indicate magnesium toxicity.The nurse should assess the client’s deep tendon reflexes frequently and report any decrease or absence of reflexes, which indicates toxicity.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today