A nurse is assessing a client who is at 39 weeks of gestation and determines that the fetus is in a left occipitoanterior position. On which of the following sites should the nurse place the external fetal monitor to hear the point of maximum impulse of the fetal heart rate?
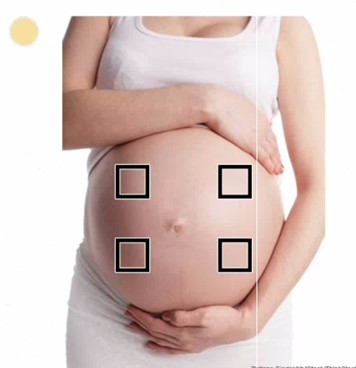
Right upper quadrant
left upper quadrant
left lower quadrant.
right lower quadrant.
The Correct Answer is C
A. This would be appropriate if the fetus were in a breech presentation.
B. This is incorrect because the fetal back is in the lower left quadrant, not the upper quadrant.
C. In the Left Occipitoanterior (LOA) Position, the fetal occiput (back of the head) is facing the mother’s left side and anteriorly (toward the front of the uterus). The fetal back will be on the left side of the maternal abdomen, making the PMI in the left lower quadrant. The best location to place the fetal monitor is over the fetal back, closest to the head. Since the fetus is cephalic (head down) in LOA position, the heart sounds are heard in the left lower quadrant.
D. This would be appropriate if the fetus were in a right occipitoanterior (ROA) position, but in LOA, the back is on the left.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is choice D. Urine output of 20 mL/hr is a manifestation of an adverse reaction to magnesium sulfate. Magnesium sulfate is a medication used to treat preeclampsia, a potentially life-threatening condition that can occur during pregnancy. Adverse reactions to magnesium sulfate include hypotension, respiratory depression, and decreased urine output. The nurse should monitor the client's vital signs and urine output closely while the client is receiving magnesium sulfate. Normal urine output in a healthy individual should be between 0.5-1.5 mL/kg/hour, and patients should generally be urinating at least every 6 hours.
Correct Answer is ["A","C"]
Explanation
A. Labor induction with oxytocin: The use of oxytocin for labor induction can increase the risk of postpartum hemorrhage due to uterine atony, where the uterus fails to contract effectively after delivery.
B. History of human papillomavirus: A history of human papillomavirus does not directly increase the risk of postpartum hemorrhage.
C. Vacuum-assisted delivery: Instrumental deliveries, such as those using a vacuum, are associated with an increased risk of trauma to the birth canal, which can contribute to postpartum hemorrhage.
D. Newborn weight 2.948 kg (6 lb 8 oz): A newborn weight of 2.948 kg is within the normal range and does not by itself increase the risk of postpartum hemorrhage. Larger babies (macrosomia) are more commonly associated with an increased risk.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today