A nurse is assessing a 64-year-old African-American client who has jaundice. The patient has a past medical history of alcoholism and liver cirrhosis. Which of the following areas is the most reliable for the nurse to inspect for jaundice?
Conjunctiva
Sclera of the eye
Back of the neck
Palms of the hands
The Correct Answer is B
Choice A Reason:
The conjunctiva can sometimes appear yellow in individuals with jaundice; however, it is not the most reliable area to inspect for jaundice. The conjunctiva may be affected by other factors such as environmental irritants or infections, which can alter its appearance.
Choice B Reason:
The sclera of the eye is the most reliable area to inspect for jaundice. The yellowing of the sclera, also known as scleral icterus, is a key indicator of jaundice. The sclera's white background provides a clear contrast, making any yellow discoloration more noticeable. This is particularly true in darker-skinned individuals, where skin changes may be less apparent.
Choice C Reason:
The back of the neck is not a reliable area to inspect for jaundice. Skin pigmentation and lighting can affect the visibility of yellowing, making it an unreliable indicator. Additionally, the back of the neck may have other skin changes unrelated to jaundice that could confuse the assessment.
Choice D Reason:
The palms of the hands are not the most reliable area to inspect for jaundice. While the palms may show yellowing, they are subject to various external factors such as manual labor or exposure to substances that can affect their color. Moreover, the palms' skin may be thicker and less transparent, making subtle changes in color more difficult to detect.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice a reason:
Immunization schedules are typically considered a part of primary prevention. They are intended to prevent diseases before they occur by using vaccines to provide immunity against infections.
Choice b reason:
Regular mammogram screenings are a form of secondary prevention. They are used to detect breast cancer lesions early before symptoms appear, which can lead to more effective treatment and better outcomes.
Choice c reason:
The consistent use of seat belts is a primary prevention strategy. It is a proactive measure to prevent injuries in the event of a motor vehicle accident.
Choice d reason:
Annual vision examinations can be considered part of secondary prevention if they are used to detect vision problems or eye diseases in their early stages. However, they can also be seen as primary prevention because they help maintain and protect eye health before issues arise.
Correct Answer is B
Explanation
Choice A reason:
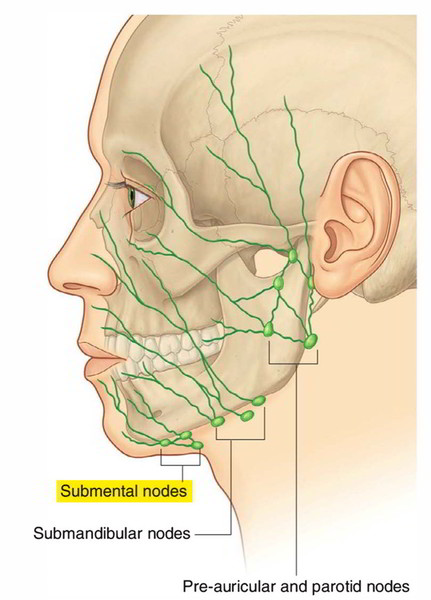
Palpating in front of the ear would assess the preauricular lymph nodes, not the submental lymph nodes. The preauricular nodes are located just in front of the ears and are typically examined when there is an infection or inflammation in the eyes, ears, or scalp.
Choice B reason:
The submental lymph nodes are located in the midline, just under the chin, behind the bony prominence of the mandible. This is the correct area for palpation when assessing the submental lymph nodes. These nodes drain the lower lip, the floor of the mouth, the tip of the tongue, and the incisors, and they can become enlarged due to infections or malignancies in these areas.
Choice C reason:
Palpating superficial to the sternomastoid would assess the cervical lymph nodes, specifically the anterior cervical nodes, which are not the submental lymph nodes. The sternomastoid muscle is a landmark for several lymph node groups in the neck, but not for the submental group.
Choice D reason:
Palpating at the angle of the mandible would assess the submandibular lymph nodes, not the submental lymph nodes. The submandibular nodes are located beneath the jawline and can become enlarged due to infections or malignancies in the mouth, throat, and salivary glands.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today