A nurse is administering a client's morning oral medications.
Which of the following actions should the nurse take?
Verify the medication three times with the medication administration record.
Document medication administration prior to administering medication.
Administer time-critical medication 60 min before or after the scheduled time.
Identify the client by using one identifier before giving the medication.
The Correct Answer is A
a. Verify the medication three times with the medication administration record.
When administering oral medications, the nurse should verify the medication three times with the medication administration record to ensure that the correct medication is being given to the correct client at the correct time. This is known as the "three checks" and is an important step in preventing medication errors.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Before any invasive procedure, it is essential to ensure that the client has provided informed consent. Informed consent involves providing the client with information about the procedure, its risks, benefits, and alternatives, allowing them to make an informed decision about their healthcare. The nurse should verify that the client has been adequately informed about the esophagogastroduodenoscopy procedure and has given consent before proceeding.
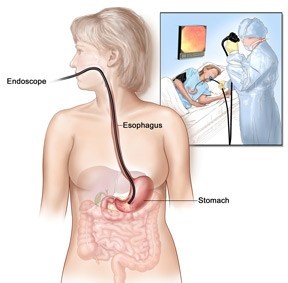
Informing the client about the procedure duration of 60 minutes is not a priority action. While it is helpful to provide the client with information about the procedure, the specific duration of the procedure may vary depending on various factors, and it does not require immediate attention prior to the procedure.
Ensuring that the client's bladder is full is not necessary for an esophagogastroduodenoscopy procedure. The procedure involves examining the upper gastrointestinal tract and does not involve the bladder or urinary system.
Administering an oral contrast solution is not typically required for an esophagogastroduodenoscopy procedure. Oral contrast solutions are commonly used for other
diagnostic imaging procedures, such as computed tomography (CT) scans or barium studies, but not for esophagogastroduodenoscopy.
Correct Answer is D
Explanation
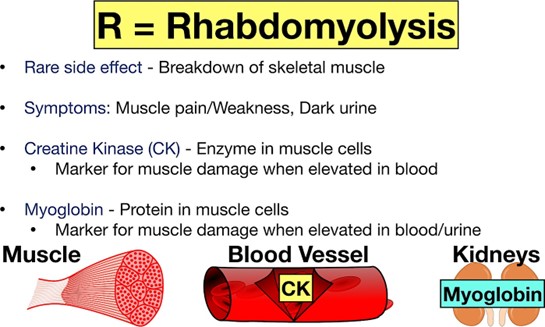
Atorvastatin is a medication used to lower cholesterol levels in the blood. One of the potential adverse effects of atorvastatin is myopathy, a condition characterized by muscle pain, weakness, and tenderness. In severe cases, myopathy can progress to rhabdomyolysis, a potentially life-threatening condition in which muscle breakdown products are released into the bloodstream and can cause kidney damage.
Therefore, the nurse should instruct the client to monitor for muscle pain, weakness, or tenderness and report these symptoms to the healthcare provider immediately. Hypoglycemia, palpitations, and daytime drowsiness are not commonly associated with atorvastatin use and would not require immediate reporting to the healthcare provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today