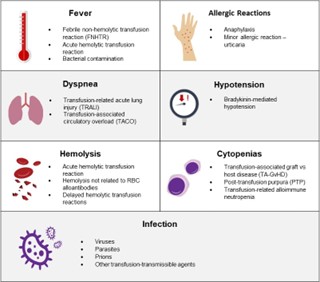
A nurse is administering a blood transfusion to a client. After 15 minutes, the client reports difficulty breathing. What is the first action by the nurse?
Stop the transfusion.
Notify the health care provider of the client s response.
Check the client s vital signs.
Document the findings.
The Correct Answer is A
Difficulty breathing is a sign of a potential transfusion reaction. When a client reports difficulty breathing during a blood transfusion, the nurse should stop the transfusion immediately to prevent the reaction from worsening. Once the transfusion is stopped, the nurse can then assess the client's vital signs and notify the healthcare provider of the client's response. Documentation of the findings should also be completed after the client's condition has stabilized. However, stopping the transfusion takes priority over documenting the findings.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
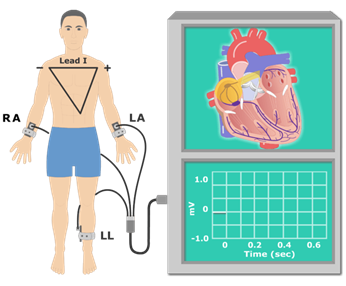
This response provides the patient with accurate and reassuring information about the EKG procedure. It explains that the test is painless and describes what will happen during the test. The other responses do not provide as much information or reassurance to the patient.
Correct Answer is A
Explanation
Deep breathing or "diaphragmatic breathing" is a technique used to prevent recurrent pneumonia and improve lung function. During deep breathing, the patient is instructed to inhale deeply, expanding their lung volume as much as possible. This process is called inspiration.
Expiration, on the other hand, is the process of exhaling or breathing out air from the lungs. Intake refers to the process of taking in air or breathing in, while chest is a part of the body where the lungs are located.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today