A nurse in the emergency department is assessing a client who has internal injuries from a car crash. The client is disoriented to time and place, diaphoretic, and his lips are cyanotic. The nurse should anticipate which of the following findings as an indication of hypovolemic shock?
Widening pulse pressure
Increased heart rate
Increased deep tendon reflexes
Pulse oximetry 96%
The Correct Answer is B
Choice A Reason: This is incorrect. Widening pulse pressure is not a sign of hypovolemic shock, but rather of increased intracranial pressure or aortic regurgitation. Hypovolemic shock causes narrowing pulse pressure due to decreased stroke volume and increased peripheral resistance.
Choice B Reason: This is correct. Increased heart rate is a sign of hypovolemic shock, as the body tries to compensate for the decreased blood volume and cardiac output by increasing the heart rate and contractility.
Choice C Reason: This is incorrect. Increased deep tendon reflexes are not a sign of hypovolemic shock, but rather of hyperreflexia or tetany. Hypovolemic shock causes decreased deep tendon reflexes due to reduced perfusion and oxygenation of the muscles and nerves.
Choice D Reason: This is incorrect. Pulse oximetry 96% is not a sign of hypovolemic shock, but rather of normal oxygen saturation. Hypovolemic shock causes decreased pulse oximetry due to hypoxia and impaired gas exchange.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
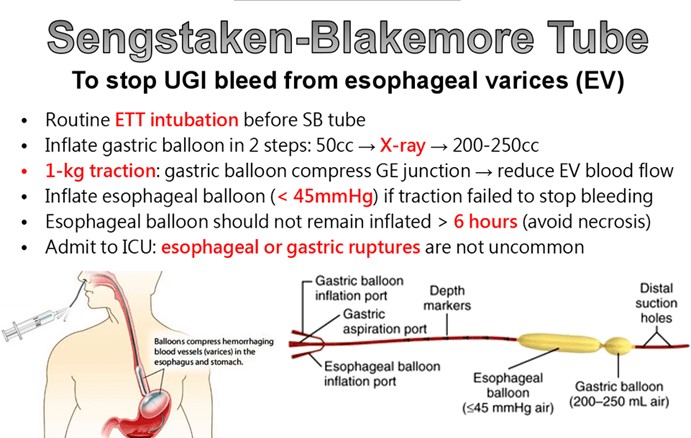
Choice A Reason: This is incorrect. The balloons should not be deflated without a physician's order, as this can cause rebleeding or aspiration.
Choice B Reason: This is incorrect. The head of the bed should be elevated to 30 to 45 degrees to reduce pressure on the balloons and prevent gastric reflux.
Choice C Reason: This is correct. The nurse should monitor the client closely for signs of complications, such as airway obstruction, aspiration, or balloon rupture. The nurse should also keep scissors at the bedside to cut the tube and release the balloons in case of an emergency.
Choice D Reason: This is incorrect. The tube should not be suctioned, as this can damage the mucosa and cause bleeding. The nurse should only aspirate gastric contents through the gastric lumen to decompress the stomach.
Correct Answer is C
Explanation
The correct answer is: C. Continue the rate at 125 mL/hr.
Choice A: Slow the rate to 50 mL/hr
Slowing the IV fluid rate to 50 mL/hr is not appropriate for a patient with a head injury. Adequate fluid management is crucial to maintain cerebral perfusion pressure and prevent secondary brain injury. Reducing the rate to 50 mL/hr could lead to hypovolemia, which might decrease cerebral perfusion and worsen the patient’s condition.
Choice B: Slow the rate to 20 mL/hr
Slowing the IV fluid rate to 20 mL/hr is even less appropriate. Such a low rate would likely result in significant hypovolemia, severely compromising cerebral perfusion pressure. This could exacerbate the patient’s head injury by reducing the blood flow to the brain, leading to further damage.
Choice C: Continue the rate at 125 mL/hr
Continuing the rate at 125 mL/hr is appropriate. This rate helps maintain euvolemia, which is essential for ensuring adequate cerebral perfusion pressure in patients with head injuries. Maintaining a stable fluid rate helps prevent both hypovolemia and hypervolemia, both of which can negatively impact intracranial pressure and cerebral perfusion.
Choice D: Increase the rate to 250 mL/hr
Increasing the IV fluid rate to 250 mL/hr is not recommended. Overhydration can lead to increased intracranial pressure, which can be detrimental to a patient with a head injury. Excessive fluid administration can cause cerebral edema, worsening the patient’s condition.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today