A nurse in an urgent care facility is assessing a client who is currently receiving outpatient treatment for anorexia nervosa. Which of the following client data should indicate to the nurse that the client requires acute care admission?
Blood pressure 78/60 mm Hg
Weight loss 20% over last 6 months
Apical pulse rate 50/min
Body temperature 35.5° C (95.9°F)
The Correct Answer is D
Choice A rationale:
A blood pressure of 78/60 mm Hg is indicative of hypotension which is a common complication of anorexia nervosa. However. the low body temperature takes precedence
Choice B rationale:
Weight loss of 20% over the last 6 months is concerning but may not be an immediate indicator for acute care admission.
Choice C rationale:
An apical pulse rate of 50/min is bradycardia, which can be a result of anorexia nervosa, but it may not be an immediate indicator for acute care admission unless the client is symptomatic.
Choice D rationale:
A body temperature of 35.5°C (95.9°F) is below a normal range signfyng hypothermia which needs immedate intervention.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
Newborns typically lose some weight after birth, but 15 percent loss would be excessive and concerning. A normal weight loss range is about 5 to 10 percent.
Choice B rationale:
Newborns should be fed on demand rather than adhering to strict schedules to ensure they are adequately nourished.
Choice C rationale:
Breastfeeding requires additional energy, and mothers are generally advised to consume around 500 extra calories a day to support milk production and their own energy needs.
Choice D rationale:
Offering a pacifier before sleep can reduce the risk of sudden infant death syndrome (SIDS), but this recommendation usually starts at around 1 to 2 months of age.
Correct Answer is C
Explanation
Choice A rationale:
Ankle swelling can be a common symptom of pregnancy and is not necessarily indicative of a complication.
Choice B rationale:
Gums can become more sensitive during pregnancy, leading to bleeding while brushing teeth. This finding is common and not necessarily indicative of a complication.
Choice C rationale:
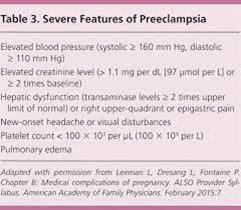
Constant pain in the middle of the upper abdomen can be a sign of preeclampsia, a serious pregnancy complication that requires prompt medical attention.
Choice D rationale:
Feeling dizzy when lying flat on the back (supine hypotension) can be a common discomfort during pregnancy due to pressure on the vena cava. However, it does not necessarily indicate a complication in this context.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today