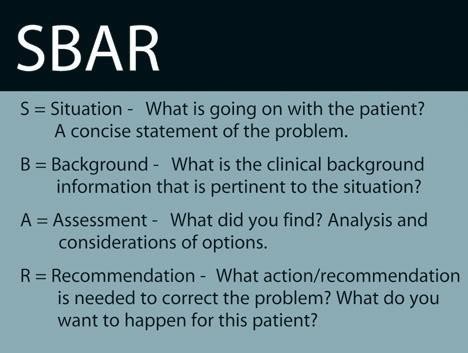
A male client who fell at home and experienced a brief loss of consciousness becomes increasingly confused after admission to the medical unit. The family requests an update on the client's condition. Using the SBAR (Situation, Background, Assessment, Recommendation) communication, which information should the nurse provide first?
Increasing confusion of the client.
Client's healthcare power of attorney.
Currently prescribed medications.
Fall at home as reason for admission.
The Correct Answer is A
Choice A Reason: This is the best action because it describes the current situation of the client and alerts the family to a possible change in the client's status. The nurse should provide the most relevant and urgent information first using the SBAR communication.
Choice B Reason: This is not the first action because it does not address the current situation of the client. The nurse should verify the client's healthcare power of attorney, but this is not a priority at this time.
Choice C Reason: This is not the first action because it does not explain the cause of the client's confusion. The nurse should review the client's medications and assess for any adverse effects, but this is not a priority at this time.
Choice D Reason: This is not the first action because it provides background information that is not directly related to the current situation of the client. The nurse should give a brief history of the client's admission, but this can be done later.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: Ensuring the transfer of the client's electronic chart code is not the most important action for the nurse to take first. The electronic chart code is a unique identifier that allows access to the client's health records and care plan. While this is an important task, it is not as urgent or essential as giving a detailed report to the accepting nurse, who will be responsible for providing palliative care to the client.
Choice B Reason: Giving a detailed report to the accepting nurse is the most important action for the nurse to take first. The report should include the client's diagnosis, prognosis, pain level, medication regimen, preferences, goals, and psychosocial needs. This will ensure continuity of care and facilitate a smooth transition for the client and the family.
Choice C Reason: Taking the family to the client's new room is not the most important action for the nurse to take first. The family may need emotional support and guidance during this difficult time, but they also need accurate and timely information about the client's condition and care plan. The nurse should first give a detailed report to the accepting nurse and then accompany the family to the new room.
Choice D Reason: Giving the client written information about end-of-life care is not the most important action for the nurse to take first. The client may benefit from learning more about palliative care, hospice care, advance directives, and bereavement services, but this should be done after giving a detailed report to the accepting nurse and ensuring that the client is comfortable and stable in the new room.
Correct Answer is D
Explanation
Choice A Reason: Managed healthcare plans do not pay for any in-hospital medical evaluations is not the best information for the nurse to provide this family. This statement is false and misleading. Managed healthcare plans may cover in-hospital medical evaluations if they are deemed medically necessary and authorized by the plan. The nurse should not discourage the family from seeking appropriate care for their mother based on inaccurate information.
Choice B Reason: Healthcare costs are escalating because clients want to have diagnostic testing conducted in the hospital is not the best information for the nurse to provide this family. This statement is irrelevant and insensitive. Healthcare costs are influenced by many factors, such as technology, inflation, regulation, and demand. The nurse should not blame the clients for wanting to have diagnostic testing done in the hospital, which may be essential for their health and well-being.
Choice C Reason: The client is grieving normally in response to her husband's death and hospitalization is not necessary is not the best information for the nurse to provide this family. This statement is presumptuous and dismissive. Grief is a complex and individual process that may affect people differently. The nurse should not assume that the client's confusion and disorientation are normal signs of grief, which may mask underlying medical conditions that require evaluation and treatment.
Choice D Reason: Managed care providers have mandatory pre-certification requirements for hospitalization is the best information for the nurse to provide this family. This statement is factual and helpful. Pre-certification is a process by which managed care providers review and approve proposed hospital admissions, procedures, or services before they are performed. The nurse should inform the family that they need to obtain pre-certification from their mother's plan before admitting her to the hospital, or they may face denial of coverage or higher out-of-pocket costs.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today