A home health care nurse is conducting a fall risk assessment for a client who has osteoarthritis and lives alone. The nurse should identify that which of the following factors creates a risk for falls?
Large pieces of furniture.
A bedside table next to the bed.
Raised toilet seats.
Throw rugs on hardwood floors.
The Correct Answer is D
Choice A rationale:
Large pieces of furniture do not necessarily create a significant risk for falls unless they are poorly placed or obstructing pathways. While they can potentially cause accidents, the likelihood of tripping over them is generally lower compared to other hazards.
Choice B rationale:
A bedside table next to the bed is not a significant fall risk factor. In fact, having a bedside table can be beneficial for the client, as it provides a convenient surface for placing items that the client might need during the night.
Choice C rationale:
Raised toilet seats, although they may pose a challenge for individuals with mobility issues, are typically installed to aid those with difficulty sitting down or standing up. They are not a primary risk factor for falls, especially when compared to other more hazardous factors.
Choice D rationale:
Throw rugs on hardwood floors are a significant fall risk factor, especially for older adults or individuals with mobility problems. The rugs can easily shift or bunch up, causing someone to trip and fall. Hardwood floors can also become slippery, and the combination of a throw rug on such a surface increases the risk of accidents. The rationale behind this choice is grounded in the potential for tripping and slipping hazards that these throw rugs can introduce, especially in individuals who might already have balance or mobility issues.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","D","E"]
Explanation
Choice A rationale:
Measuring the amount of aspirate in the NG tube is one way to verify the placement of the tube. Aspirate should be tested for color, pH, and other characteristics to ensure proper positioning.
Choice B rationale:
Flushing the tube with tap water doesn't directly verify tube placement. This action might inadvertently introduce air into the tube, potentially leading to inaccurate assessment results.
Choice C rationale:
Examining the color of aspirated secretions is an essential step in verifying tube placement. Different colors of aspirate can indicate different anatomical locations, helping to ensure the tube is properly positioned.
Choice D rationale:
Measuring the pH of the client's aspirate is another important method to verify NG tube placement. Gastric aspirate tends to be acidic, while respiratory aspirate is usually more alkaline.
Choice E rationale:
Obtaining an x-ray of the client's chest and abdomen is a definitive method for confirming NG tube placement. It provides direct visualization of the tube's location and ensures accuracy.
Correct Answer is B
Explanation
Choice A rationale:
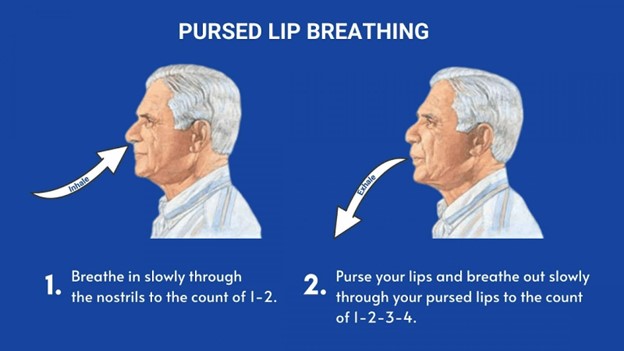
Lying down while practicing pursed-lip breathing is not the correct instruction. Pursed-lip breathing is usually performed in a sitting or standing position. Lying down can restrict lung expansion and may not effectively support the purpose of this breathing technique, which is to improve airway pressure and reduce air trapping.
Choice B rationale:
"Exhale slowly through your mouth" is the correct instruction for pursed-lip breathing. This technique involves inhaling through the nose for a count of two and exhaling slowly and steadily through pursed lips for a count of four. The goal is to promote better exhalation, prevent airway collapse, and improve oxygen exchange. The rationale behind this choice is grounded in the mechanics of pursed-lip breathing, which helps create backpressure in the airways, maintaining them open and aiding in proper exhalation.
Choice C rationale:
Inhaling through pursed lips contradicts the proper sequence of pursed-lip breathing. The technique involves inhaling through the nose and exhaling through pursed lips. Inhaling through pursed lips would not provide the intended benefits of the technique.
Choice D rationale:
"Puff your cheeks when exhaling" is not the correct instruction. Puffing the cheeks during exhalation does not contribute to the effectiveness of pursed-lip breathing. This action could potentially impede proper exhalation and defeat the purpose of the technique, which is to control airflow and improve breathing efficiency.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today