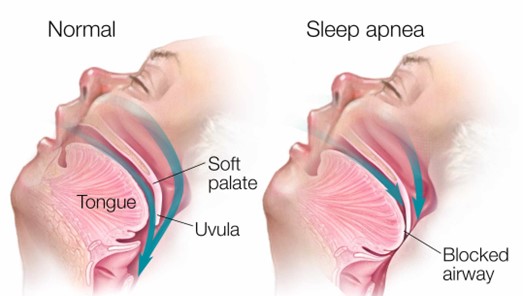
A client with obstructive sleep apnea (OSA) ambulates in the hallway with the nurse prior to bedtime and then returns to bed. Which intervention is most important for the nurse to implement before leaving the client?
Apply the client's positive airway pressure device.
Elevate the head of the bed to a 45 degree angle.
Remove dentures or other oral appliances.
Lift and lock the side rails in place.
The Correct Answer is A
Choice B reason: Elevating the head of the bed to a 45-degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as a positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C","E","F"]
Explanation
Choice B is correct because weight management is an important factor in preventing and controlling hypertension. Taking daily walks for thirty minutes can help reduce weight and lower blood pressure.
Choice C is correct because salt substitutes can help with maintaining a healthy diet by reducing sodium intake. Sodium intake is associated with increased blood pressure and should be limited to less than 2,300 mg per day.
Choice E is correct because sodium intake can be regulated by rinsing canned foods in water. Canned foods often contain high amounts of sodium as a preservative and rinsing them can remove some of the excess sodium.
Choice F is correct because uncontrolled hypertension can lead to renal damage. Hypertension can cause damage to the blood vessels and impair the function of the kidneys, leading to chronic kidney disease or failure.
Choice A is incorrect because alcohol consumption can produce vascular changes that increase blood pressure. Alcohol intake should be limited to no more than one drink per day for women and two drinks per day for men.
Choice D is incorrect because blood pressure readings should not be taken at noontime. Blood pressure readings should be taken at the same time each day, preferably in the morning before breakfast or in the evening before dinner.
Correct Answer is B
Explanation
Choice A: An abdominal binder can be worn daily to reduce the protrusion is not a correct explanation for the nurse to provide, as this is not an effective or recommended method to treat a hernia. This is a distractor choice.
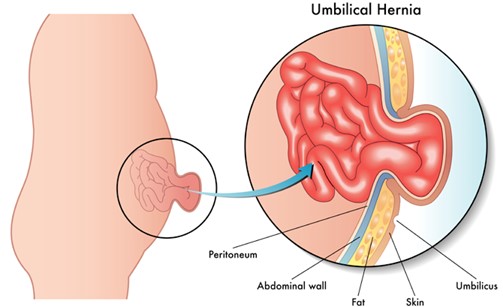
Choice B: This hernia is a normal variation that resolves without treatment is a correct explanation for the nurse to provide, as this refers to an umbilical hernia, which is a common and harmless condition in infants that usually disappears by age 2. Therefore, this is the correct choice.
Choice C: The quarter should be secured with an elastic bandage wrap is not a correct explanation for the nurse to provide, as this is a folk remedy that has no scientific basis and can cause skin irritation and infection. This is another distractor choice.
Choice D: Restrictive clothing will be adequate to help the hernia go away is not a correct explanation for the nurse to provide, as this is not a proven or safe way to treat a hernia. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today