A client whose hyperthyroidism has not been responsive to medications is admitted for evaluation. During the admission assessment the client reports to the nurse of a sudden onset of feeling apprehensive and nurse notes the client is restless and very warm to touch. Which action should the nurse implement next?
Access laboratory results to confirm a thyroid crisis.
Obtain a complete set of vital signs.
Initiate intravenous access.
Encourage relaxation and slow deep breathing.
The Correct Answer is C
In this scenario, the client's sudden onset of feeling apprehensive, restlessness, and increased body temperature are consistent with symptoms of a thyroid crisis, also known as thyroid storm or thyrotoxic crisis. Thyroid crisis is a life-threatening condition that requires immediate medical intervention.
Initiating IV access is crucial to ensure the prompt administration of medications and fluids to manage the thyroid crisis effectively. IV access allows for the administration of beta-blockers, antithyroid drugs, and supportive care, which are essential components of the treatment for thyroid crisis. IV access also provides a route for fluid resuscitation if necessary.
Accessing laboratory results to confirm a thyroid crisis is important, but the clinical presentation of the client with sudden onset symptoms and a known history of uncontrolled hyperthyroidism suggests the need for immediate intervention rather than waiting for laboratory confirmation.
Obtaining a complete set of vital signs is an important assessment to gather comprehensive data, but in the case of a suspected thyroid crisis, immediate intervention takes precedence over obtaining vital signs.
Encouraging relaxation and slow deep breathing may be beneficial in managing anxiety or discomfort, but it does not address the underlying emergency situation of a thyroid crisis. The nurse should focus on initiating appropriate medical interventions first.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","C","E"]
Explanation
A) Correct- Assessing the child's pulse helps determine their cardiac status and whether they have a detectable heartbeat. This information is essential for deciding the appropriate interventions.
B) Correct- Placing a cervical collar is necessary if there is any suspicion of cervical spine injury due to the fall or submersion. This action helps stabilize the neck and prevent further damage to the spine.
C) Correct- Checking for open wounds is important to assess for potential sources of bleeding or infection that may require immediate attention.
D) Incorrect- While child safety is important, the immediate priority in this situation is assessing and stabilizing the child's medical condition. Child protective services may be involved later if there are concerns about the circumstances surrounding the incident.
E) Correct- Assessing the airway is of utmost importance to ensure that the child can breathe. In cases of near-drowning, ensuring a clear airway is crucial for oxygenation.
F) Incorrect- While establishing intravenous access may be important for certain interventions, it is not one of the immediate priorities in this situation. Ensuring the child's airway, breathing, and circulation take precedence.
Correct Answer is A
Explanation
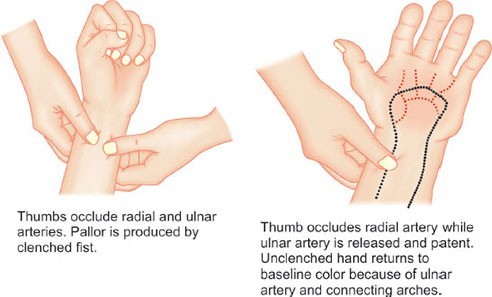
Allen's test is a procedure used to assess the patency of the ulnar artery and the collateral circulation of the hand. It is performed to determine the adequacy of collateral circulation before obtaining arterial blood gases from the radial artery. The test helps ensure that the ulnar artery is functioning properly and can supply blood to the hand if the radial artery is used for blood sampling or other invasive procedures.
The test involves occluding both the ulnar and radial arteries while the patient clenches their fist. The nurse then releases pressure on the ulnar artery while maintaining occlusion of the radial artery. The hand should quickly regain normal coloration, indicating adequate collateral circulation.
It's important to note that the Allen's test is specific to the assessment of collateral circulation in the hand and is not used for other purposes such as assessing deep vein thrombosis, cardiac output calculation, or obtaining pulmonary artery pressures.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today